In the first part of this series, I examined how fallacious reasoning and indirect methods commonly used by virologists can deceive them into believing they’ve found a “virus” when no such thing has been demonstrated.
I focused on the case of Dr. Robert Shihman Chang and the so-called “lipovirus,” a phenomenon that arose in 1954 when artificial cytopathic effects (CPE) were observed during early cell culture experiments. These effects were interpreted as evidence of a “transmissible cytopathic agent.” Instead of first purifying and isolating any presumed “viral” particles, researchers attempted to retroactively fit the observed effects to the “viral” hypothesis.
Despite the absence of purified, isolated, photographed, and characterized “viral” particles, Dr. Chang and others pursued serological tests in an attempt to establish a “viral” identity—claiming that this presumed “virus” existed both in those sick with hepatitis and in the general population via the detection of “antibodies.” However, any contradictory evidence—particularly findings that did not conform to the predetermined expectations of what a “virus” should be—was ignored or dismissed.
Eventually, independent research revealed that the observed CPE was not caused by a “virus” at all, but by an ameboid. What had been considered evidence of a “viral” cause turned out to be a case of mistaken identity. Dr. Chang ultimately accepted this reinterpretation, and the “viral” hypothesis collapsed.
This case stands as a damning example of how a researcher can deceive himself through circular reasoning and indirect, assumption-laden evidence—constructing an imaginary cause on a foundation lacking scientific rigor. Yet, this was not an isolated incident.
Around the same time the “lipovirus” was being investigated, Japan faced a severe neurological outbreak. This debilitating condition was marked by the degeneration of the spinal cord, optic nerve, and peripheral nerves, and led to widespread panic and misattribution of cause—much like in the “lipovirus” case.
The clinical features included:
Progressive weakness and numbness in the legs, sometimes leading to paralysis
Visual impairment or blindness due to optic neuritis
Loss of reflexes and sensation in affected areas
Urinary and fecal incontinence
Cognitive changes and alterations in personality
Symptoms typically developed over weeks to months, sometimes leading to severe disability or even death if left untreated. In the early stages, the condition was mistaken for benign encephalomyelitis, multiple sclerosis, polio, or Devic's disease. In fact, it was once called “Non-specific encephalomyelitis with abdominal symptoms” due to the lack of unique or distinguishing symptoms. The question was even posed as to whether or not the disease “constitutes a distinctive clinicopathological entity, since it is well documented that a variety of neurological disorders may be accompanied by acute abdominal conditions.” However, as clinical and post-mortem evidence accumulated, it was decided that this was a distinct disease, marked by “unique,” non-inflammatory degenerative damage to the nervous system. In 1965, the term Subacute Myelo-Optico-Neuropathy (SMON) was proposed to capture these features and its unknown cause, quickly gaining acceptance for its clarity and utility.
Several hypotheses were proposed to explain this seemingly new disease, including:
Intoxication from agricultural pesticides, industrial waste, or heavy metals
Excessive or improper drug use
A metabolic disorder or vitamin deficiency
A neuro-allergic condition, suggested by the sex and age distribution
An “infectious” etiology
Unsurprisingly, the “infectious” hypothesis gained the most traction—an outcome this article will focus on. It was widely considered the most plausible explanation at the time. As part of the investigation, multiple researchers claimed to have found “cytopathic agents” in the spinal cord, cerebrospinal fluid, blood, and feces of SMON patients. This gave rise to a wave of confidence that a new “virus” would be uncovered.
In the early 1970s, virologist Shigeyuki Inoue emerged as the leading proponent of the “viral” hypothesis for SMON, relying on the usual indirect and ultimately unconvincing pseudoscientific lines of evidence. His claims gained traction not because they were conclusive, but because they aligned with prevailing assumptions in a field dominated by “virus-centric” thinking. At the time, Japan was still heavily invested in polio research, and many of the same virologists simply redirected their focus toward SMON. Inoue’s findings—examined in detail below—were seen as legitimizing to the search for a “viral” cause. Yet in the end, the very data meant to support the theory helped dismantle it. As this article will show, SMON is not merely an embarrassing footnote in medical history—it is a revealing case study in how institutional bias, scientific inertia, and the allure of the invisible “virus” can not only derail reason and prolong suffering, but also enable a culture of deception to masquerade as medical certainty.
"I was at that time engaged in poliovirus research, so I suspected such a virus to be the cause."
-Reisaku Kono
The SMON episode began in Japan around 1955, when patients started reporting numbness or loss of sensation in the feet following bouts of gastrointestinal illness. These early symptoms were accompanied by impaired vision and difficulty walking due to progressive paralysis in the lower limbs. By 1957, large outbreaks of the polio-like condition were reported across Japan, leading many to suspect a “contagious” cause. However, the disease’s nonspecific presentation created diagnostic confusion, particularly during Japan’s polio outbreak between 1960 and 1961. Although SMON was eventually considered unrelated to polio, it was sometimes referred to as “adult polio” due to the similarity in symptoms and the overlap in timing with polio epidemics of the 1960s.
According to the paper Subacute myelo-optic neuropathy and cioquinol: An epidemiological case-history for diagnosis, abdominal symptoms nearly always preceded the neurological ones. However, deaths from the disease were difficult to track, as SMON was frequently associated with other conditions. It was estimated that no more than 5% of patients actually died from SMON itself.
The primary neurological differential diagnosis was subacute combined degeneration (SCD) of the spinal cord. SMON also shared overlapping features with multiple sclerosis, pernicious anemia, various intestinal disorders (such as blind loops, strictures, and anastomoses), Coeliac disease, and toxic exposures to lead, mercury, arsenic, and thallium. In its “less complete forms”—typically marked by abdominal symptoms and dysesthesia—SMON was difficult to distinguish from other causes of peripheral neuropathy and myelopathy. Since these “incomplete forms” accounted for the majority of cases, misdiagnoses were common and posed serious challenges to epidemiological investigation.
For nearly the entire course of the epidemic—from 1955 to 1970—SMON was widely believed to be an “infectious” disease. This belief was primarily supported by a consistent summer peak in incidence, reports of clustering among individuals who drank fecally contaminated water from the same sources, and claims by various researchers that they had isolated microbiological “pathogens” from affected patients.
Subacute myelo-optic neuropathy and cioquinol
An epidemiological case-history for diagnosis
THE DISEASE, AND A SUSPECTED CAUSE
During the mid- and late 1950s, doctors in Japan were consulted by increasing numbers of patients with an unusual combination of alimentary and neurological complaints. The common clinical picture was of abdominal pain and/or diarrhoea, followed within a few days or weeks by painful dysaesthesiae; in addition to the predominantly sensory disturbances, upper and/or lower motor neurone signs occurred in just over 50% of cases, and visual disorders due to optic neuritis in about 28% (Sobue et al., 1971). The disease was called subacute myelo-optic neuropathy, or SMON. Table I summarizes Kono's (1971) list of SMON's 'cardinal' and other symptoms; of particular importance is that the abdominal symptoms nearly always preceded the neurological. Case-fatality from SMON itself is hard to assess because the disease was very often associated with other conditions, many having a poor prognosis; but it is likely that not more than 5% of SMON patients actually died of the disease itself. On the other hand, probably 90 % of patients were left with dysaesthesiae, and 50% with limb weakness, visual impairment, or both; 10 to 15% were completely disabled (Kono, 1971). By the time the epidemic was over, some 10 000 Japanese were said to have developed SMON, a figure of the same order as the world wide total of thalidomide-deformed children. The main epidemiological features of the disease are summarized in Table II; these have not been seriously contested by the protagonists or antagonists of the hypothesis on aetiology with which this review is concerned.
Subacute combined degeneration (SCD) of the cord is the main neurological differential diagnosis of SMON; multiple sclerosis has also to be considered. In addition to pernicious anaemia, SCD may, of course, be associated with a number of intestinal disorders resulting in impaired vitamin B12 adsorption-such as blind loops, strictures, and anastomoses.Coeliac disease, lead, mercury, arsenic, and thallium intoxications also give rise to both abdominal and neurological manifestations, so that SMON was by no means unique in these respects. Neurologists are in general agreement that SMON exhibiting all its neurological features, visual, motor, and sensory, was a distinct and real clinical syndrome, but it is clear that in its less complete forms it was not easily distinguishable from other causes of peripheral neuropathy and myelopathy. Since these incomplete forms (for example, abdominal symptoms and dysaesthesiae) accounted for most cases, opportunities for misdiagnosis were frequent, a fact with obvious implications for epidemiological studies.
For virtually the whole course of the epidemic, which ran from 1955 to 1970, SMON was regarded as probably being an infectious disease (Ogata and Jitsunari, 1970). The main points in favour of an infective aetiology were a regular summer peak in incidence, and claims that the disease clustered in individuals drinking faecally contaminated water from the same source. Various workers (see Kono, 1971) claimed to have identified or isolated microbiological pathogens. The newness of the disease, its predilection for the elderly rather than the young, and the absence of expected clinical and pathological features of infective disease (for example, in the cerebrospinal fluid) were reasons against the infective theory.
In his book Inventing the AIDS Virus, virologist Peter Duesberg recounted how the SMON epidemic in postwar Japan became a cautionary tale of scientific misdirection. He highlighted how the research establishment, dominated by virologists, approached the disease with a rigid assumption: SMON had to be “infectious.” This untested premise shaped the entire investigation, leading “virus” hunters to fixate on identifying the “right virus” while largely ignoring or downplaying evidence that challenged the idea of “contagion.”
Assuming that the disease was “infectious,” researchers jumped to conclusions to confirm their assumptions. Clusters of cases in families and hospitals were taken as confirmation of “transmissibility,” despite the lack of clear transmission pathways or consistent patterns. The seasonal spike in cases during late summer even prompted speculation about insect vectors. Meanwhile, early “non-infectious” hypotheses—such as exposure to environmental toxins or occupational hazards—were pushed aside, not because they were falsified, but because they didn’t fit the dominant paradigm.
As Duesberg observed, this kind of misplaced attribution—blaming microbes for conditions that may not be “contagious” at all—was not new. What made SMON notable was how long the “viral” theory persisted, despite mounting evidence to the contrary. For over a decade, the assumption of a “viral” cause went unchallenged as the framework discouraged exploration of other possibilities, despite a lack of compelling evidence.
Duesberg recounted how, in May 1964—after years of uncertainty surrounding the polio-like disease—SMON became a formal topic of discussion at the 61st General Meeting of the Japanese Society of Internal Medicine. During this meeting, researchers officially named the condition Subacute Myelo-Optico-Neuropathy (SMON) and agreed upon standardized diagnostic criteria. A formal research commission was soon launched by the Japanese Ministry of Health and Welfare, led by Kyoto University professor Magojiro Maekawa. Among the virologists appointed to the commission was Reisaku Kono, a prominent figure in Japan's virology community, effectively cementing a presupposed “viral” etiology as the guiding assumption. The very structure of the investigation had been front-loaded with that assumption: they were not asking whether the disease was “viral”—they were tasked with identifying which “virus” was responsible.
The first major “breakthrough” came from Masahisa Shingu, a virologist at Kurume University and fellow commission member, who claimed in 1965 to have found an “echovirus”—a type of “enteric virus” first discovered during polio research—in the excretions of SMON patients. Based on this, Shingu asserted he had found evidence of “infection” and concluded that this “orphan virus” had finally been matched with a disease. He enthusiastically published his findings, boasting that he had “isolated” the cause of SMON.
But the logic was flawed from the start. When subsequent researchers, including Kono himself, failed to replicate these findings or demonstrate “infection” in patients, the “virus” hypothesis should have been abandoned. Instead, it lingered—not because of evidence, but because virology had become too institutionally committed to its own presumptions. Another wave of excitement followed in 1968, when two researchers reported the presence of a “Coxsackie virus”—another class of “enteric virus,” also discovered incidentally during polio research—in SMON patient tissue. This too was later debunked, as the “discovery” turned out to be the result of accidental laboratory contamination.
The supposed presence of “enteric viruses” in some patients was taken as causative proof—a textbook case of affirming the consequent: “If a virus caused SMON, we’d expect to find it in patients. We found one—therefore, it must cause SMON.” That leap, combined with the absence of proper controls and a refusal to entertain “non-viral” hypotheses, fueled years of misguided research. The SMON episode is often treated as an embarrassing historical footnote—but it actually reveals something deeper: a field so embedded in its own framework that it confuses assumptions for evidence.
“Viruses” were not the only suspects considered in the search for SMON’s cause. Bacterial explanations were also explored, though with similarly circular logic and inconclusive results. Some researchers noted imbalances in the intestinal flora of SMON patients, but no novel or invasive microbe was ever identified. Even when high levels of mycoplasma—a genus of bacteria commonly present in healthy individuals—were detected, the findings were dismissed as incidental. Kono’s lab, along with two others, reported these unusual concentrations, but because mycoplasma are frequently found in the general population and typically associated only with minor or unrelated conditions like pneumonia, the trail was abandoned.
Rather than prompting a re-evaluation of the broader assumption that SMON must have an “infectious” cause, these dead ends were treated as mere setbacks in an otherwise unquestioned paradigm. The failure to identify any “novel virus” or bacterium wasn’t taken as a reason to challenge the foundational belief—it simply meant the “right pathogen” hadn’t been found yet.
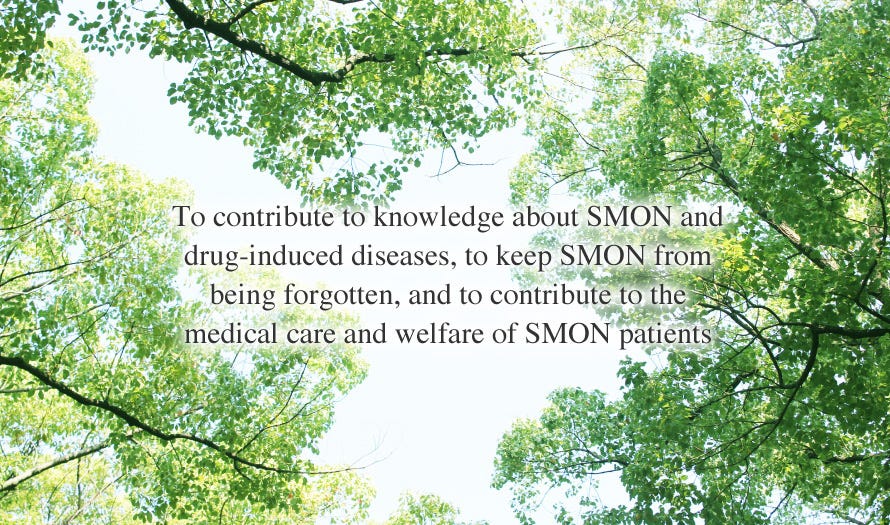
The persistent effort to find a causative “pathogen” culminated in a claim by Assistant Professor Shigeyuki Inoue—from Kyoto University’s Institute for Virus Research—who reported discovering a herpes-like “virus” in SMON patients in his paper Virus Isolated from Patients of Subacute Myelo-Optico-Neuropathy (SMON) in Japan. His findings were summarized in a short communication published in The Lancet, where he stated that the “virus” was isolated with “high frequency” in BAT-6 hamster tumor cells, showing “weak and incomplete” cytopathic effects (CPE). However, attempts to isolate the “virus” with accompanying CPE in HeLa cells, primary monkey-kidney cells, and human embryonic-kidney cells were unsuccessful.
Inoue claimed that antiserum prepared from the isolated “virus” could neutralize CPE produced not only by other “viruses” in stool but also by “viruses” found in spinal fluid from SMON patients. Despite this, he explained the absence of high titres of “neutralizing antibodies” in patient sera by pointing to the disease's subacute and relapsing course. Inoue suggested that the “virus” might be a new “neuropathic slow virus” responsible for SMON, citing pathological findings such as spongy degeneration in the brain in mice “infected” with the “virus.”
Virus Associated with S.M.O.N in Japan
Sir,—In recent years many patients in Japan have acquired subacute myelo-optico-neuropathy (S.M.O.N.) following abdominal disorders. At present its aaiology is not known; however, among the etiological hypotheses is that of Professor Tsubaki and his colleagues (April 3, p. 696)—that S.M.O.N. may be a toxic reaction to oral administration of clioquinol—and a viral theory. We describe here the isolation and some properties of a suspect virus present in stools and spinal fluid of S.M.O.N. patients.
Virus was isolated, with a high frequency, in BAT-6 cell-cultures with accompanying weak and incomplete cytopathic effect (C.P.E.) from feces and spinal fluid of S.M.O.N. patients living in different prefectures, as shown in the accompanying table. Attempts to isolate the virus accompanying C.P.E. in hela cells, primary monkey-kidney cells, and human embryonic-kidney cells were all unsuccessful. On the other hand, no virus was isolated in BAT-6 cells from control specimens except in two adult cases of aseptic meningitis. Antiserum prepared from the virus isolated from feces neutralised not only the C.P.E. produced by the other viruses from the stool but also the C.P.E. produced by all viruses from the spinal fluid of S.M.O.N. patients.
Neutralising-antibody (N.T.) titres of 13 of 15 sera collected from S.M.O.N. patients on different days after the onset of the disease were 5-10. In contrast, 10 sera collected from normal adults showed N.T. titres of less than 5. The apparent absence of high titres in patients sera may explain the subacute and relapsing course of the disease. Furthermore, convalescent sera from 2 patients with aseptic meningitis showed N.T. titres of 160 to 320. This suggests that S.M.O.N. may be a new viral infection which succeeds immunological insufficiency.
BAT-6 cells have not proved susceptible to the human enteroviruses so far tested, and the virus showed a characteristic host range in tissue-culture. The virus was sensitive to ether and idoxuridine. Also, the virus was filtrable through a membrane filter with an average pore-size of 22 mu, but could not pass through a 100 mu-pore filter. Studies on the pathogenicity of the virus in mice suggest that the virus is a new neuropathic slow virus; the pathological findings include spongy degeneration in the brain. Further investigations about the properties of the virus are now in progress.
Inoue’s study suffered from several critical flaws that undermined the validity of his claims. First, his alleged “virus” could only be “isolated” in BAT-6 mouse lymphoma cells—an abnormal, non-human cell line—while standard human and primate cell lines, including HeLa, monkey kidney, and embryonic kidney cells, failed to yield any “viral” replication or cytopathic effects. This suggested that the observed results were most likely cell line-specific artifacts or due to contamination, rather than evidence of a genuine human “pathogen.” The cytopathic effects themselves were described as “weak and incomplete,” raising further doubts about their specificity or biological relevance. Additionally, the study lacked consistent serological evidence: SMON patients did not exhibit the expected high levels of “neutralizing antibodies.” Rather than interpreting this as a contradiction of the “viral” hypothesis, Inoue speculated—without direct evidence—that the low titers were due to the “subacute and relapsing” nature of the disease. This circular reasoning substituted assumptions for proof.
Moreover, the criteria used to infer the presence of a “virus”—such as ether sensitivity, idoxuridine inhibition, and filtration—were not supported by direct visualization or molecular characterization of any “viral” particle. The only image accompanying his initial study showed cytopathic effects claimed to be caused by a “virus” without any direct purification, isolation, and visualization of any “virus-like” particles.
The use of oversized membrane filters (22 μm and 100 μm) further muddled the conclusions, as these pore sizes are not considered appropriate for detecting “known viruses,” which are typically much smaller. Claims of “pathogenicity” in mice were vague and based on nonspecific signs such as “spongy degeneration” in the brain, with no clear demonstration of causality or reproducibility. Most critically, the study failed to fulfill even basic standards of virological proof, such as Koch’s Postulates or adequate control experiments, and did not demonstrate actual transmission of disease. Taken together, these methodological shortcomings showed that Inoue’s findings were speculative at best and ultimately served to prolong the virological misdirection over the cause of SMON.
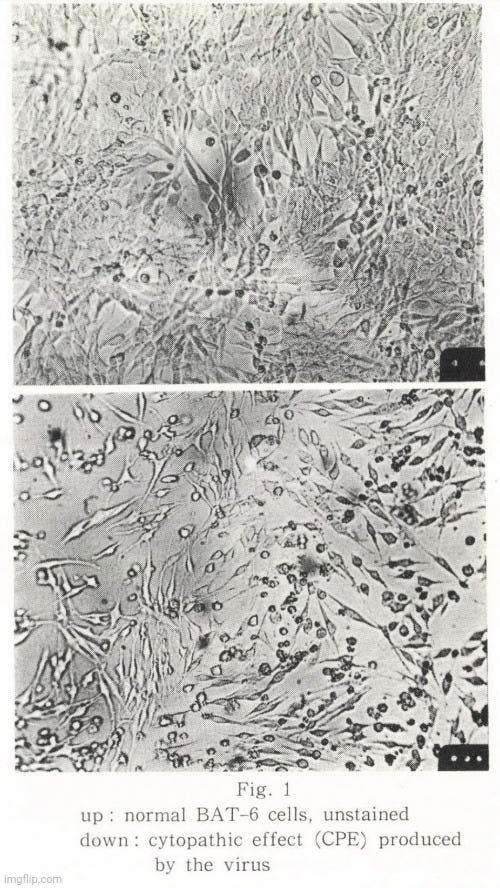
Regardless, the new “virus” trail continued in December 1970 with a paper by Zensuke Ota titled Electron Microscopic Demonstration of a New Virus Isolated from a Patient with SMON that described the first electron-microscopic observation of Inoue's alleged “virus.” Ota claimed that the morphological and developmental characteristics suggested this was a “new type” of “virus” not previously “isolated” from humans, and he presumed it to be the causative agent of SMON. The observed “virus-like” particles, he noted, closely resembled the mouse leukemia “virus” morphologically. He also cited epidemiological surveys from the Yubara district of Okayama Prefecture as support for the belief that SMON was most likely an “infectious” disease caused by a “virus.”
Interestingly, Ota acknowledged that several “known viruses” had previously been “isolated” from SMON patients and claimed as causative agents, yet none had yielded positive results in confirmation studies. Inoue’s report of cytopathic effects in cultured cells exposed to a Millipore-filtered extract of a patient's feces was taken as evidence of successful “viral isolation.” Inoue supplied Ota with a sample of this alleged “virus,” which Ota used in a replicated cell culture process. For electron microscopy, cells displaying cytopathic effects 4 to 6 days after “infection” were collected, fixed with glutaraldehyde and osmium tetroxide, and embedded in Epon for sectioning.
However, the electron microscopy observations described in the study are fundamentally flawed and fail to demonstrate the presence of a “virus.” The interpretation rests entirely on assumption, not evidence. Structures described as “virus particles” were identified purely by appearance, using terms like “budding,” “envelope,” and “nucleocapsid” as if their meaning were self-evident. No biochemical purification, characterization, or demonstration of “infectivity” was performed to confirm the identity of these particles. The sizes of the observed particles—ranging from 100 to 140 nanometers—were inconsistent, and their shapes were variable, making it entirely plausible that they were simply cellular debris, vesicles, or “exosomes,” all of which are commonly present in cultured cells.
Crucially, no effort was made to purify or isolate these particles directly from patient fluids or even from the culture supernatant. The sample used was a mixture of unknowns, and electron microscopy was applied to unpurified material. Underscoring this lack of rigor, Ota reported the presence of mycoplasma—ubiquitous contaminants known to alter cellular morphology and induce changes such as vacuolization and membrane budding, which can mimic “viral” effects. These contaminants were not controlled for. Ota also admitted that “virus-like” particles were rare, particularly the mature forms, and none were found in control cells. Such rarity is inconsistent with a productive and “pathogenic viral infection.”
Electron Microscopic Demonstration of a New Virus Isolated from a Patient with SMON
DISCUSSION
The virus particle observed in the present study closely resembles mouse leukemia virus in the morphological aspect. However, the followings are the characteristics of the present virus different from leukemia virus. The mature virus particle in this study has a denser nucleoid, the formation of which is completed before its release from the pedicle. According to INOUE'S study (5), this virus shows a clear cytopathogenic effect and is analysed to be DNA in nucleic acid type. The formation process of this virus virion is muchmore similar to Japanese encephalitis virus, since the nucleoid of both viruses is completed before their release from cells (6).
Although broad studies on this virus have not yet been accumulated, it is consiqered that this virus can be a causative agent of SMON. As for mycoplasma, it is presumed that this might be a passenger microorganism, since in many known morbid conditions, mycoplasma has been isolated merely as a passenger (7).
Ultimately, this study demonstrates how visual assumptions and narrative bias can masquerade as scientific evidence. Without proper isolation, purification, and functional validation, these EM images serve only as speculative illustrations—not proof of a “virus.”
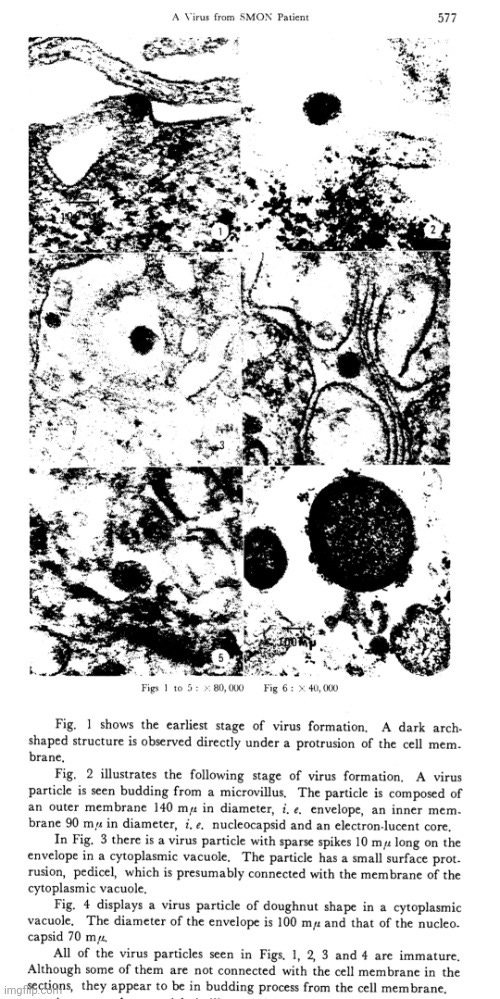
In the 1971 article The Aetiology of S.M.O.N., Professor Inoue gave an update on his ongoing search for a “viral” cause of the condition. He reported that progress was being made and cited as an important development the susceptibility of C57BL/6 mice to the presumed “virus” when inoculated intracerebrally at birth. However, this is a major methodological flaw. Injecting unpurified material directly into the brains of newborn mice does not constitute evidence of “viral pathogenicity.” This highly artificial and traumatic procedure bypasses all natural routes of exposure, and any resulting symptoms—such as stunted growth or underdevelopment, paralysis, or death—could be due to cellular debris, toxins, or contaminants, not a “virus.”
Inoue further claimed that the “virus” had been successfully “isolated” in human diploid cells, despite the fact that these cells showed no cytopathic effect—a key marker often used to infer “viral” activity. The lack of cytopathic changes, coupled with the absence of purification and characterization, offers no concrete evidence that a “virus” was replicating. Nevertheless, the researchers still classified this as a successful isolation, revealing a strong confirmation bias. They also reported that the “virus” could be isolated directly in mice using unpurified spinal fluid from SMON patients, which again raises the same concerns: unpurified samples contain a mix of biological materials that could independently cause neurological damage or stress responses in mice. Without strict controls, such as using spinal fluid from non-SMON patients under identical conditions, these findings are speculative at best.
The Aetiology of S.M.O.N.
Sir,—In regard to the progress of our virological work on S.M.O.N., we are glad to communicate that our studies are proceeding successfully. One of the recent important observations was that C57BL/6 mice were found to be susceptible to the virus isolated from S.M.O.N. patients. DD and CF1 strains of mice were less susceptible. The virus isolated in BAT-6 cells (hamster tumour cells) produced disease in C57BL/6 mice when inoculated intracerebrally at birth, after an incubation period of more than 2-3 weeks. Infection was evidenced by runting, paralysis, and death (see figure). To eliminate the possibility that the virus came from the tumour cells, human diploid cells were employed for isolation of the virus. The virus was observed to multiply in human diploid cells without cytopathic effect, and the virus isolated in human diploid cells also produced disease. Furthermore, we succeeded in isolating the virus directly in C57BL/6 mice with spinal fluid from S.M.O.N. patients shown to have the virus at more than 10⁵ T.C.D₅₀ per 0.1 ml. as determined by BAT-6 cell-cultures. The lesions in mice are under investigation; usually non-inflammatory degeneration was present in the nervous system. The properties of the virus and its pathogenicity will be published in full later.
Inoue also attempted to dismiss the increasingly accepted clioquinol toxicity theory—which held that SMON was caused by poisoning from the widely used antimicrobial drug—by pointing to geographic and epidemiologic observations. He noted that SMON cases had not been reported outside Japan, despite the global use of clioquinol, and that roughly 14.8% of Japanese patients had not reported taking the drug. However, this line of reasoning is weak. Variations in drug dosage, formulation, prescribing practices, or underreporting could easily account for these discrepancies. The fact that new SMON cases were reported even after clioquinol was suspended does not negate its role either—residual drug use, misdiagnosis, or unrelated neuropathies could explain such cases.
As Inoue wrote:
“Against the clioquinol theory is the fact that no S.M.O.N. patients have been reported outside Japan, although clioquinol is taken in many other countries. In contrast, there have been approximately 10,000 cases of S.M.O.N. in Japan, and it is reported that 14.8% of the patients had taken no clioquinol. Furthermore, new cases of S.M.O.N. have appeared since the suspension of clioquinol in Japan.”
Ultimately, Inoue’s conclusions reflect a pattern of assuming a “viral” cause despite insufficient and uncontrolled evidence. The “virus” remained hypothetical, propped up by ambiguous interpretations, poorly controlled experiments, and an apparent reluctance to accept the far more plausible explanation: drug-induced toxicity.
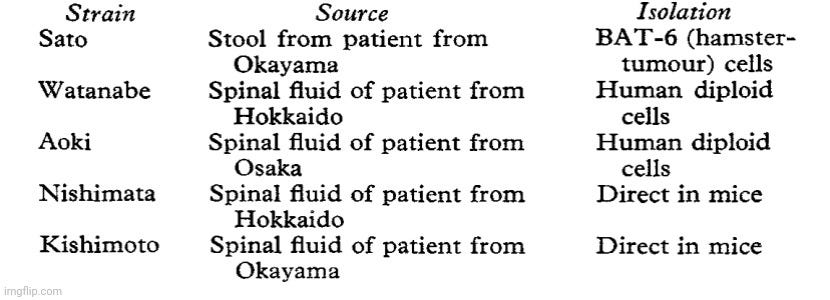
In January of 1972, Inoue published the paper Pathogenicity of virus associated with subacute myelo-optieo-neuropathywhich reiterated much of what he explained in the proceeding article relating to the death of newborn mice upon intracerebral injection. However, there were some interesting details to note. The “Materials and Methods” section described how strains of the supposed SMON “virus” (Watanabe and Aoki strains) were prepared using the method of Nishibe and Inoue that were unpublished at the time, presenting a transparency problem. Without a published method, the protocol cannot be scrutinized or replicated. The supernatant from culture fluids was used after low-speed centrifugation (5000 rpm for 30 minutes), which is not sufficient to isolate or purify presumed “viral” particles. This preparation likely contained a mix of cell debris, proteins, and potential contaminants—not just “viral” particles. However, this was never investigated as no attempts were made to check purity via the electron microscope.
In addition, the practice of naming multiple “virus strains” (Watanabe, Aoki, Nishimata, Kishimoto) based solely on vague and unpurified preparations implies a veneer of scientific rigor without any real substance. No biochemical characterization or demonstration of transmissibility was provided.
Pathogenicity of virus associated with subacute myelo-optieo-neuropathy
Materials and Methods
Virus materials.—The source of the five strains of virus was as follows:
The Watanabe and Aoki strains were isolated by the method of Nishibe and Inoue (to be published). The supernatant portion of the culture fluid was used after centrifugation at 5000 r.p.m. for 30 minutes. For isolation of the virus directly in C57BL/6 mice (Nishimata and Kishimoto strains), spinal fluid of S.M.O.N. patients was used which contained more than 10⁵ TCID₅₀ per 0.1 ml, as determined with BAT-6 cells.
As mentioned previously, even more concerning is the method used for “isolation” in mice: spinal fluid from SMON patients, allegedly containing >10⁵ TCID₅₀ per 0.1 ml, was injected directly into the brains of newborn mice. This intracerebral route of inoculation is highly artificial and bypasses all normal barriers of “infection.” It introduces a foreign, unpurified biological mixture directly into the central nervous system of extremely vulnerable newborn animals. Any number of factors—such as protein aggregates or residual drug compounds—could cause neurological damage or death. This is not valid evidence of “viral infection” or “pathogenicity.”
Moreover, the criteria for assessing outcomes are not described here—only that mice were observed for two months and those that died within the first week were excluded from results. Excluding early deaths can bias the results and obscure the possibility that the material was acutely toxic rather than “infectious.” While controls are mentioned in the paper, what was done to the controls was left undescribed. There was no mention of whether or not the controls were injected with spinal fluid from healthy individuals or filtered culture medium, which is a glaring omission. Without such controls, any observed symptoms in the test group are uninterpretable.
Mice.—Newborn mice of dd, C57BL/6, and CFl strains were used. Viral materials were inoculated intracerebrally at birth. The inoculated mice were observed for two months. Mice which died within one week were excluded from the results. C57BL/6 mice were kindly supplied by Dr. A. Ishimoto, Aichi Cancer Center Research Institute, and Dr. M. Maeda of our institute.
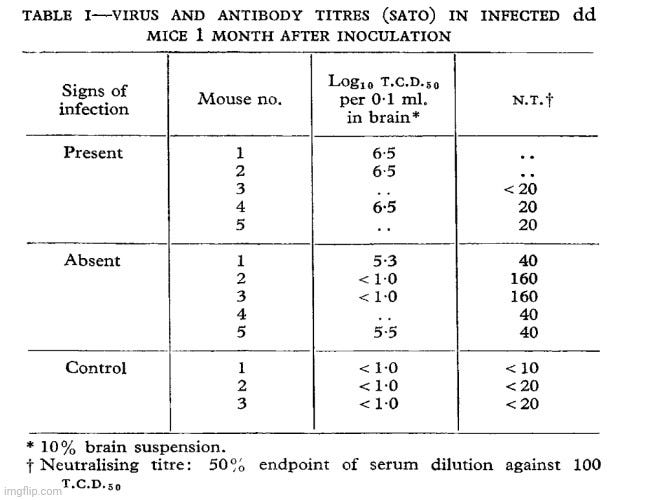
Out of 66 mice injected intracerebrally at birth with the “Sato strain,” only 9 showed abnormal signs such as wasting, ruffled hair, or hydrocephalus, while all 27 CF1 mice were completely unaffected. This casts doubt on the claim of “consistent pathogenicity.” More importantly, the data in Table I reveal that even among the symptomatic mice, only a few showed detectable “viral” titers in brain tissue, and only two exhibited any “neutralizing antibody” response. Several symptomatic mice had no detectable “virus” or “antibodies,” while some asymptomatic mice did show relatively high “antibody” titers or detectable “virus.” This inconsistency undermines the claim that a “viral infection” was present or causative. The “control” mice, as expected, showed no signs of “infection” and had no “viral” titers or significant “neutralizing antibodies.” However, the mere presence of control animals without “infection” does not compensate for the erratic and inconclusive findings among the test subjects.
Adding to the problem, the researchers admitted that susceptibility to disease varied significantly between litters and that the “infectious” titer of the agent was difficult to determine. They also noted that “uninfected” culture fluid and preparations neutralized with “immune” serum failed to produce disease, further complicating the interpretation.
Sato strain.—Only 9 out of 66 dd mice inoculated intracerebrally at birth showed abnormal signs (wasting, ruffling of hair, hydrocephalus), and all 27 of the CFI mice were unaffected. The susceptibility of the dd mice seemed to differ between litters. The relation between the virus titre in brain and the neutralising-antibody titre in serum of the infected dd mice was examined one month after inoculation, and the diseased mice proved to have high virus titres in the brain and low antibody titres in the serum; mice which showed no signs of infection had a lower virus titre and a higher antibody titre (table 1).
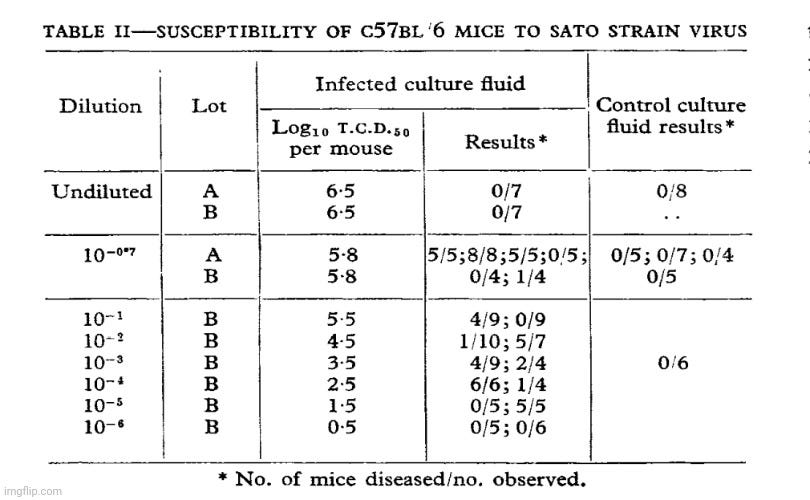
In Table II, results are presented that, rather than supporting a clear-cut “viral infection” model, raise serious concerns about experimental consistency and the validity of the interpretation. When undiluted “infected” culture fluid—presumably containing the highest concentration of the “virus”—was injected into mice, none of them developed disease (0/7 in both lots A and B). This is striking because if a “virus” were responsible, the highest dose should result in the highest rate of disease. By contrast, when the same fluid was diluted down to 10⁻⁷—a ten-million-fold dilution—nearly all mice developed signs of disease (e.g., 5/5, 8/8, 5/5). This inversion of the expected dose-response pattern is biologically implausible and suggests an alternative explanation, such as toxicity or some other experimental artifact at play.
As the culture fluid was diluted further (from 10⁻¹ through 10⁻⁶), results remained erratic and inconsistent. Some dilutions showed partial disease induction (e.g., 4/9 at 10⁻¹, 6/6 at 10⁻⁴), while others showed little to no effect. These irregular patterns do not reflect a predictable or reproducible “infectious” process. Meanwhile, all “control” culture fluid samples—presumably “uninfected” but otherwise treated similarly—produced no disease across all dilutions, suggesting that only the so-called “infected” material triggered the effects, though not in a logically consistent manner.
In short, this table does not provide convincing evidence of a “pathogenic virus.” The fact that undiluted samples caused no disease while diluted ones sometimes did contradict the basic expectations of “viral” behavior. These findings are more consistent with uncontrolled variables, toxic byproducts, or preparation artifacts than with infection by a replicating “viral” agent.
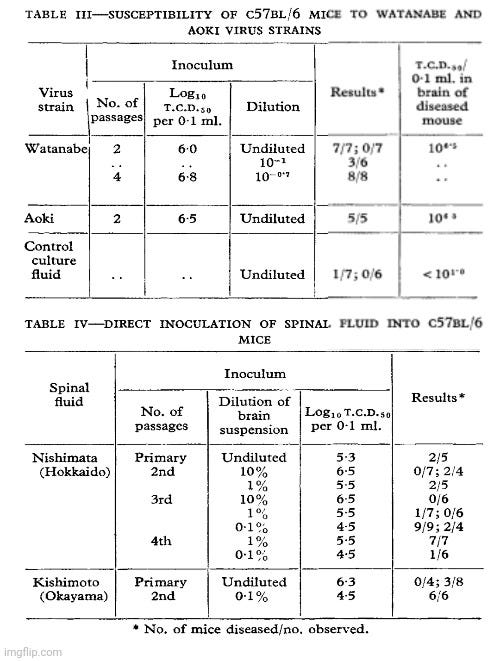
As mentioned previously, the “controls” used in these experiments are weak and poorly defined. While a “control culture fluid” is referenced in Tables II and III, the authors do not clearly describe how this fluid was prepared or whether it underwent the same procedures, passages, or handling as the so-called “infected” material. Without this information, it’s impossible to determine whether the control is a valid comparison. Compounding the issue, one of the seven mice given control fluid still developed disease symptoms, suggesting that factors other than a “virus” are responsible for the observed effects.
In Table IV, more inconsistent and ambiguous results were presented showing that some mice that received undiluted or highly concentrated material showed no signs of disease, while other mice exposed to far more diluted inoculant exhibited widespread illness. Again, this lack of a coherent dose-response relationship would be uncharacteristic of a specific “infectious agent” and instead points to the influence of random variation, experimental noise, or “non-viral” factors such as toxins or inflammation.
The increasing T.C.D₅₀ values across successive passages in culture—such as from 6.0 to 6.8 in the Watanabe strain—are often interpreted as evidence of “viral replication.” However, this interpretation is flawed, as passaging may merely concentrate unknown toxic substances or amplify other biological contaminants without proving that a “virus” is being replicated. The higher “titer” could just as easily reflect an accumulation of harmful byproducts rather than a rise in “infectious viral particles.”
Finally, the reliance on T.C.D₅₀ as a metric is a form of circular reasoning. This measure assumes that the observed cytopathic effects (CPE) in tissue culture are caused by a “virus.” But if the CPE arises from toxicity, cell stress, or other “non-viral” causes—as has not been ruled out here—then using T.C.D₅₀ as evidence for a “virus” is merely presupposing what the experiment is supposed to demonstrate. It’s not proof of a “virus;” it’s an assumption built into the method itself.
Altogether, this study lacks the necessary rigor to support the conclusion that a “virus” was isolated or proven to cause SMON. The erratic results, lack of purification, and reliance on invasive methods reveal more about the researchers’ assumptions than they do about the existence of a “viral pathogen.”
In September 1972, Inoue published another response in The Lancet titled Antibody Response in Cases of S.M.O.N. Against the Associated Virus. While he tried to use the results of serological testing to confirm his “viral” hypothesis, his claims relied on speculative reasoning, weak evidence, and circular logic.
Antibody Response in Cases of S.M.O.N. Against the Associated Virus
Sir,—We have reported that subacute myelo-optico-neuropathy (S.M.O.N.) may be a viral infection which succeeds immunological insufficiency. The agent can produce a similar disease in C57BL/6 mice, and seems to be a new neuropathic virus. We describe here the antibody response of patients with S.M.O.N. to the associated virus.
First, Inoue highlighted that “convalescent sera showed an increased antibody titre,” suggesting this is indicative of “viral infection.” However, he acknowledged that the sera were taken from patients more than 12 months after peak illness. This long delay makes it unclear whether the elevated “antibody” titers had anything to do with the disease or were simply due to unrelated “immune” activity over time. The lack of acute-phase data severely limits the interpretability of the “antibody” measurements.
Convalescent sera showed an increased antibody titre (see table). Because the course of the disease is subacute, the convalescent sera were chosen from patients in whom more than 12 months had elapsed since the peak of the disease or the last recurrence. The accompanying figure gives sequential results in a case of S.M.O.N., showing the course of clinical symptoms and a subsequent gradual increase in the neutralising-antibody titre during convalescence.
Inoue claimed that three out of six nurses who cared for SMON patients had detectable “antibodies” which was interpreted as evidence of “inapparent infection.” But this conclusion assumes the very thing that needs to be proven: that the presence of “antibodies” reflects a specific, transmissible “viral” exposure related to SMON. In reality, “antibody” detection is regularly demonstrated to result from nonspecific cross-reactivity or even laboratory artifacts. No causal link was demonstrated.
Inoue also mentioned that three cases of aseptic meningitis showed high “antibody” titers from which they reportedly “isolated” the SMON “virus” from spinal fluid. But again, the logic is circular. They argue that the presence of “antibodies” and the claimed “virus isolation” confirm the “virus” caused the meningitis—but both the “antibody” interpretation and the “virus” identification rely on prior assumptions that the “virus” exists and is causative, as well as the existence of specific “antibodies” to it. The statement that “no other virus could be isolated” does not eliminate “non-viral” causes or prove that the isolated agent is “pathogenic.” It simply reflects the limitations of their methods.
Sera from 3 of 6 healthy nurses who looked after the S.M.O.N. patients had antibody. This indicates that inapparent infection may occur. Convalescent sera from 3 cases of aseptic meningitis showed high antibody titres. The serum of 1 case was tested at an early stage of the disease, but its titre was less than 10. From this and the positive results of S.M.O.N. virus isolation from the spinal fluids these cases of aseptic meningitis were judged to be due to S.M.O.N. virus. No other virus could be isolated from the spinal fluids. In 71 of 73 control sera from normal adults, antibody titres were less than 10.
Inoue's conclusion—that the “serological evidence” supports the hypothesis that SMON is due to “infection” with a “novel virus”—rests heavily on assumptions rather than direct proof. No electron microscopy or purified “virus” is shown. No reproducible disease is demonstrated via exposure with an “isolated virus” in animals or humans. No demonstration of transmissibility from one host to another was directly shown. The assertion that the “virus” persists due to “immunological insufficiency” is speculative and unfalsifiable, serving as a convenient explanation for inconsistent or delayed “immune” responses. The suggestion that the SMON “virus” could cause different neurological diseases depending on the “host/virus relationship” added even more ambiguity, effectively shielding the hypothesis from disproof by allowing for nearly any outcome.
These results provide serological evidence that a virus is related to S.M.O.N. and are good agreement with our hypothesis that S.M.O.N. is due to infection with a new virus following immunological insufficiency. A delayed antibody response in S.M.O.N. patients seems to result in establishment of subacute, persistent infection with S.M.O.N. virus. Therefore, it is understandable that the rate of isolation of virus from the spinal fluid of S.M.O.N. patients is unusually high (reported at approximately 80%). A state of immunological insufficiency is undoubtedly important in the pathogenesis of S.M.O.N. Our results also indicate that S.M.O.N. virus may also cause a different neurological disease, aseptic meningitis, depending on the host/virus relationship.
Inoue repeatedly begged the question—assuming a “virus” was involved in order to interpret his findings as evidence for that “virus.” He relied on poorly defined terms, ambiguous serology, unconfirmed “isolations,” and speculative “pathogenesis.” These types of claims may seem compelling at first glance, but they collapse under closer logical scrutiny.
In 1973, Inoue published the paper Properties of Virus Associated with Subacute Myelo-Optico-Neuropathy, which largely repeated findings from earlier work. However, as always, there were notable details worth highlighting. For example, in section 2.8, Inoue claimed purification of the “virus” used in his experiments. Yet despite the technical language, the process described is inherently nonspecific and leaves significant ambiguity.
Properties of Virus Associated with Subacute Myelo-Optico-Neuropathy
2.8. Concentration and Purification of Virus
Harvested virus, after centrifugating at 2000 rev./minute for I0 minutes was centrifuged at 10,000 rev./minute for 30 minutes at 4° C (GSA rotor of a Sorvall RC 2-Bcentrifuge). Virus was then sedimented by centrifugating at 28,000 rev./minute for 100 minutes (RP30 rotor; Hitachi 55P centrifuge). Each pellet was resuspended in 1 ml (0.2 % of original volume) of phosphate-buffered saline, pl-I 6.5, and dispersed with ultrasonic vibration before clarification at 5000 rev./minute for 30 minutes; this was the concentrated virus for experiments.
This procedure describes differential centrifugation at various speeds, intended to separate particles by size and density. The final product—labeled as “concentrated virus”—is the pellet formed after ultracentrifugation, which is then resuspended and sonicated. However, at no point is it demonstrated or verified that this pellet contains only a “virus,” nor is there any indication that the “virus” has been isolated in the proper scientific sense—meaning separated from all other components and shown to cause a specific, reproducible effect on its own.
In reality, this final suspension is a crude mixture likely containing cellular debris, extracellular vesicles, proteins, nucleic acids, and other substances. This is especially problematic given that the starting material—so-called “harvested virus” from cell culture—is itself a complex and undefined soup. Without additional purification steps (such as density gradient ultracentrifugation) and rigorous characterization (e.g., electron microscopy of isolated particles, proteomic profiling, or functional testing of purified fractions), there is no scientific justification for confidently labeling this material as “virus.”
Furthermore, the phrase “concentrated virus for experiments” indicates that this mixture was used in downstream assays, such as cell culture inoculation and “antibody” testing. But if the material isn't truly purified, then any observed effects (e.g., cytopathic effects in cell culture or “antibody” responses in humans or animals) cannot be conclusively attributed to a “virus.” They are more plausibly the result of toxins, cellular byproducts, or other contaminants present in the mixture.
In section 3.2, Inoue described how undiluted passage fluid—presumably containing the highest concentration of “virus”—resulted in unclear cytopathic effect (CPE) and lower “viral” yield compared to diluted passage. Even more telling is that mixing undiluted fluid with diluted fluid suppressed the yield from the latter, implying that something in the undiluted sample actively inhibits the system. Conversely, mixing diluted passage fluid with uninoculated cell extract did not suppress yield.
3.2. Effect of Dilute and Undiluted Passage on Virus Yield
As shown in Table 1, for undiluted passage, CPE in BAT-6 cells at 5 to 6 days after infection was not clear, and the virus yield was also inhibited when compared with that for dilute passage. The undiluted passage fluid suppressed the yield when mixed with the dilute passage fluid. No suppression was observed in the dilute passage mixed with unlnoculated cell extract. Thus, the low yields in undiluted passages are considered to be due to an interfering factor in undiluted fluids.
Inoue concluded that an “interfering factor” must exist in the undiluted fluids without ever identifying it, which raises serious red flags. If the material assumed to be rich in “virus” instead suppresses replication and yield, it contradicts the basic premise of “infectious viral” behavior. This phenomenon could point to toxic byproducts, degradation products, cellular debris, or other “non-viral” contaminants accumulating in the undiluted material—none of which would be expected if a clean, “replicating virus” were the active agent.
This result is not just a technical oddity—it undermines the validity of their assumptions about “viral propagation.” If increased “viral” load leads to suppression, then what’s being measured would not be a “virus” at all, but most likely a complex and unstable mixture where toxic or inhibitory factors dominate the outcome.
In section 3.3, Inoue noted that “infectivity” was greater in the culture fluid than in the cell-associated fraction, leading them to use only the culture fluid in further experiments. This raises an immediate question: if a “virus” is replicating inside cells, why would the extracellular fluid show more “infectivity” than the intracellular component? In the standard virology narrative, productive “viral replication” typically results in high intracellular “viral load,” with the “viral” particles releasing into the medium following lysis or budding. Their finding suggests that the culture fluid contains other agents (e.g., toxic cell metabolites or breakdown products) that produce effects interpreted as “infectivity” or “CPE” without any actual “viral replication” occurring.
3.3. Growth of Virus in BAT-6 Cells at 36°C
The infectivity of virus in culture fluids (Fig. 2) was increased and was higher than that of the cell-associated virus. For this reason, only infective culture fluid was used as virus for further investigation. The CPE for BAT-6 cells was observed in tube cultures but not in bottle cultures.
Second, Inoue noted that CPE was observed in tube cultures but not in bottle cultures. This is problematic because both vessel types are commonly used and should yield comparable results if the CPE is caused by a “replicating virus.” The discrepancy points to experimental conditions—and not the presence of a “virus”—driving the results. Differences in oxygenation, cell density, fluid volume, or handling could be responsible, which weakens the argument that the effects observed are due to a “virus.”
The discussion section of the paper reveals several major shortcomings in the case for a “virus” being the cause of SMON, despite Inoues’ attempts to argue otherwise.
4. Discussion
The virus associated with S.M.O.N. failed to produce CPE in human diploid cells, HeLa cells, or primary monkey kidney cells,and produced weak and in complete CPE in BAT-6 cells. Control tests with several entero-viruses (polio-viruses type 1, 2, 3; Coxsackieviruses A-9, B-l, B-3, B-5; echoviruses type 1, 2, 3, 6, 2l) failed to produce CPE in BAT-6 cells (unpublished). The physicoehemical properties of the agent suggest a DNA virus with a buoyant density of 1 21 to 1.22 g/ml, not filterable through a 100 nm Millipore filter, and sensitive to ether and FUDR. At present, only few ether-sensitive DNA viruses have been isolated from human faeces. Some properties of the virus resemble those of subgroup A of the herpesvirus group although anti-type 1 and type 2 herpesvirus immune sera failed to neutralize the infectivity of the virus (unpublished). The pathogenicity in suckling C57BL/6 mice (NAKA~V~A and INovE, 1972) also suggests a new virus. Furthermore, the characteristic pathological findings observed in Goll’s and pyramidal tracts of the spinal cord, suggest a so-called "slow virus". Further studies, particularly by electron microscopy, are needed for classification of the virus.
First, as previously reported, the so-called “virus” failed to produce CPE in human diploid cells, HeLa cells, or primary monkey kidney cells—all of which are standard, biologically relevant models used for testing “viral pathogenicity.” Even in BAT-6 cells, a hamster tumor cell line, the CPE was described as “weak and incomplete,” which raises serious doubts about the agent’s relevance and “virulence.” Additionally, Inoue claimed the agent had properties consistent with a DNA “virus”—such as a specific buoyant density and ether sensitivity—but these traits are nonspecific and could apply to a wide variety of “non-viral” cellular debris or extracellular particles.
He attempted to compare the agent to “herpesviruses” based on some shared properties, yet noted that “immune” sera against herpes simplex types 1 and 2 failed to neutralize it. This undermines the claimed similarity and suggests that the agent is either unrelated or that its characterization is fundamentally incomplete. Although Inoue cited “pathogenicity” in suckling mice as evidence of a “virus,” as already discussed, such experiments rely on artificial conditions, like intracerebral injection of unpurified material, and are not indicative of natural “infection” or human disease. Labeling the agent a “slow virus” further muddies the waters, as this term has historically been used when mechanisms are poorly understood and should not be seen as confirmation of “viral” identity. Most strikingly, Inoue conceded that electron microscopy and further studies were needed to classify the agent, a clear admission that no definitive identification or isolation had been achieved. In short, rather than providing compelling evidence of a “novel pathogenic virus,” this discussion exposed the speculative nature and weak foundations of the “viral” hypothesis for SMON.
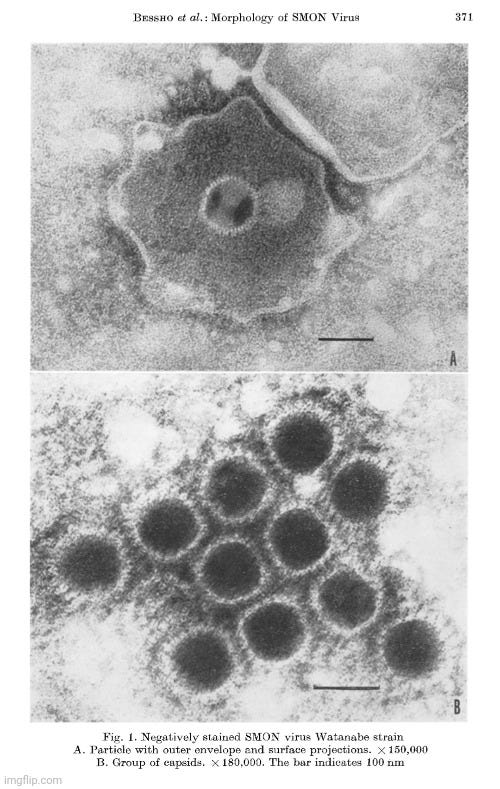
Finally, in 1974, Invoue published Morphology of SMON virus, a brief report showcasing further electron microscopy images of his presumed “virus.” He claimed that the particles observed exhibited structural features consistent with “herpesviruses,” particularly “avian infectious laryngotracheitis (ILT) virus.” Using negative staining with phosphotungstic acid and electron microscopy at 30,000–40,000× magnification, he reported seeing “virus-like” particles with morphology resembling “herpes simplex virus”—specifically, a hexagonal capsid approximately 110 nm in diameter with an arrangement of 162 capsomeres. The material used for imaging was cultivated on chorioallantoic membranes of embryonated eggs or in human diploid cells, but no purification was done, and the identification was based solely on visual resemblance. No biochemical confirmation was provided, and no causal link to SMON was demonstrated. Thus, the identification remains speculative at best, and the entire approach unscientific.
Morphology of SMON virus
The virus particles of both strains have a structure identical with those of herpes simplex virus (8) and ILT virus (2). The envelopes usually ruptured varied in size and projections were seen in profile over their surface. The capsid measured approximately 110 nm in diameter and showed hexagonal outline, as shown in Figures 1 and 2. The ring-shaped capsomeres measuring approximately 10 nm in external diameter were arranged in the form of equilateral triangles, each side consisting of 5 units, indicating a 5:3:2 rotational symmetry and a total number of 162 eapsomeres per virus particle. Thus, also in respect to its morphology, SMON virus is found to be a herpesvirus.
"We were still within grasp of the ghosts of Pasteur and Koch!"
-Reisaku Kono
Interestingly, according to Peter Duesberg, Inoue's colleague who initially claimed to have photographed the alleged “virus” using an electron microscope later retracted his report, admitting the images had been mistaken. Despite Inoue’s confidence in having discovered a “viral” cause of SMON, the indirect evidence he presented was unconvincing to many—most notably Reisaku Kono. After Inoue’s announcement, Kono tested his claims using Inoue’s own “virus isolate” and cell cultures. Within three months, he found that while the supposed “virus” could kill certain cells, those cells were highly prone to spontaneous death—even in “uninfected” controls. Kono was unable to isolate any “virus” from SMON patients and began to openly question whether the “virus” existed at all.
In a 1971 review titled Subacute Myelo-Optico-Neuropathy: A New Neurological Disease Prevailing in Japan, which summarized the current state of SMON research, Kono noted that some members of the SMON Research Commission remained committed to the “infection” hypothesis and resisted the emerging clioquinol hypothesis, which had gained traction due to research by Toyokura and his colleagues. Noticing the green tongue and urine occasionally found in SMON patients, the researchers collected a sufficient quantity of green-colored urine from two patients and identified the pigment as iron chelates of clioquinol, a drug commonly used in Japan to treat dysentery. Their findings were reported in June 1970, prompting an immediate review of patient records. This revealed that the majority of SMON patients had taken clioquinol for more than one week before the onset of neurological symptoms. In response, the Ministry of Health and Welfare banned the sale of drugs containing clioquinol in September 1970, resulting in a sharp decline in SMON cases.
As Kono pointed out, the majority of the SMON commission had come to reject a microbial cause due to a lack of convincing evidence and instead supported the clioquinol hypothesis:
“On the other hand, being convinced of the infection hypothesis, some scientists of the Research Commission are strongly opposing the clioquinol hypothesis. But no definitive microbial causative agent has ever been confirmed, although some investigators claimed to have successfully isolated echovirus type 21 and a new virus. At the moment, most of the study group believe that viral and other microbial etiology of SMON is unlikely, since there are few convincing evidences supporting virus or other microbes as the etiological agent and fitting in the clinico-epidemiological pattern of the disease.”
Several researchers aligned with Kono and failed to detect any such “virus” in SMON patients or replicate the cell damage Inoue had described. Even when using samples directly from Inoue’s lab, no one could identify a “virus.” While a few mice became ill after being injected with the material, the symptoms did not resemble SMON, further weakening the case for causality. These repeated failures to replicate Inoue’s findings raised serious doubts—not only about his conclusions, but about the very existence of the agent he claimed to have found. As in any scientific inquiry, reproducibility is essential, and its absence was a fatal flaw in the “viral” hypothesis.
Despite Kono’s methodical rebuttal, refuting the “viral” hypothesis proved difficult. Inoue had already gained national attention in early 1970, before any link to clioquinol was publicly recognized. Japanese media prematurely announced that a “virus” had been found, sparking widespread panic. Families of SMON patients avoided contact with their loved ones, fearing “contagion.” Tragically, many patients, overwhelmed by stigma and isolation, took their own lives. This hysteria made it nearly impossible for competing explanations—such as the drug toxicity hypothesis—to gain early traction.
Duesberg emphasized that the interpretation of SMON as a “non-infectious” condition never gained traction with researchers invested in a “viral” cause. The idea that clioquinol—a drug prescribed to treat gastrointestinal symptoms—might instead be the culprit met even greater resistance. Accepting such a conclusion would have forced physicians to confront the disturbing possibility that their own prescriptions were exacerbating patient symptoms, even contributing to irreversible nerve damage. Many found it easier to believe in a mysterious, invisible “virus” than face the reality that their treatment was to blame. As Totsuka remarked, doctors and scientists were inclined to believe in a “virus” simply because they had prescribed clioquinol. Constipation and abdominal discomfort—recognized side effects of the drug—were instead mistaken for early symptoms of SMON, prompting repeated and escalating doses. This created a dangerous feedback loop, where the “treatment” intensified the very condition it was meant to resolve.
Even after Inoue’s results could not be replicated, Duesberg observed that the “virus” theory took on a life of its own. SMON had emerged during Japan’s ongoing battle with polio, and many researchers—Kono included—had built their careers studying “poliovirus.” Kono stated, “I was at that time engaged in poliovirus research, so I suspected such a virus to be the cause.” It was only natural that they would gravitate toward a familiar explanation. The Japanese government, already invested in polio research, continued funding these same virologists as they redirected their attention to SMON. As a result, virology remained the dominant force—controlling research funds, media attention, and the direction of inquiry. Other groups soon reported findings similar to Inoue’s, but notably, this wave of confirmation came only after clioquinol had been banned and SMON cases had already dropped dramatically.
It was Kono’s foresight in bringing non-virologists into the commission that ultimately shifted the narrative. Without this broader perspective, the outbreak might have dragged on under the weight of a faulty hypothesis.
A December 1971 New York Times article titled Japanese Doctors Link Nerve Disease To Dysentery Drug reported that Japanese researchers had successfully induced SMON-like symptoms in dogs and cats by administering toxic doses of the dysentery drug over six months. However, editors at The Lancet cautioned that the study did not conclusively prove clioquinol as the cause and suggested that a “virus” might still play a role—possibly in combination with the drug.
Regardless, in July 1972, the SMON Research Commission convened to resolve the controversy. Given the consistent failure to replicate Inoue’s findings, the commission concluded that further research into the “virus” hypothesis was unwarranted and shifted focus to investigating clioquinol. Still, Inoue and his colleagues continued to promote the so-called SMON “virus” in subsequent publications, even managing to secure its inclusion in the 1974 edition of the Review of Medical Microbiology. As Duesberg pointed out, global enthusiasm for “virus” research at the time, which outpaced the evidence, likely contributed to the uncritical acceptance of Inoue’s claims.
In response to this persistent promotion of the “viral” hypothesis, Reisaku Kono published the letter The S.M.O.N. Virus Theory in The Lancet in August 1975 formally rejecting the theory. He outlined a comprehensive critique, highlighting the fundamental failures that undermined the claim:
Unreliable CPE Observations: The BAT-6 cell line used by Inoue was prone to spontaneous degeneration, making cytopathic effects (CPE) unreliable as indicators of “viral infection.” Thus, “infectivity” and neutralization tests based on CPE were invalid.
Failure to Isolate the Agent: Kono’s team could not isolate any “virus-like” agent from SMON patients using Inoue’s procedures.
Lack of “Antibody” Evidence: No “neutralizing antibodies” to Inoue’s “virus” were found in the sera of SMON patients.
Electron Microscopy Failures: Other scientists (Higashi, Nii, Krech) could not detect “herpes-like” particles in samples where Inoue claimed to observe them, even after immunocomplexing and ultracentrifugation.
Questionable Animal Studies: Attempts to reproduce Inoue’s claim that the “virus” caused demyelination in mice failed. Histological changes cited by Inoue were shown to occur in uninoculated mice as well and were interpreted as normal developmental features, not signs of neurovirulence.
Epidemiological Refutation: After clioquinol was banned in 1970, SMON cases rapidly declined to zero by 1974. If Inoue’s “virus” were truly “infectious” and shed as widely as claimed, the disease should have continued spreading.
The S.M.O.N. Virus Theory
SIR,—Inoue et al. published several papers on S.M.O.N. (subacute myeloopticoneuropathy) virus (Inoue agent), and a standard textbook adopted Inoue’s virus theory as confirmed. However, research in the laboratories of the S.M.O.N. Research Commission in Japan failed to confirm Inoue’s results. Unfortunately, this negative information has not been published in English, so this letter attempts to make clear our opinion, based on our search for confirmation of Inoue’s results.
One of the crucial points of Inoue’s results lies in the reading of cytopathic effect (C.P.E.) in BAT-6 cell culture infected with Inoue agent. Since the cell strain tends to degenerate spontaneously, a specific C.P.E. in BAT-6 cell inoculated with Inoue agent could not be recognised as a criterion of infection. Therefore, the endpoint of infectivity of and neutralising antibody to Inoue agent cannot be determined quantitatively. Kono et al. have been unable to isolate a C.P.E. agent from S.M.O.N. patients by Inoue’s procedure, and they could not find neutralising antibody against Inoue agent in sera of S.M.O.N. patients. Higashi, Nii, and Krech failed to find herpes-like virions in electron micrographs of ultracentrifuged materials from infected BAT-6 cells, those of ultrathin sections of infected BAT-6 cells, or of the material which should contain immunocomplexed virion by treatment of the antiserum against Inoue agent.
Nakamura and Inoue reported that they had transmitted the disease to suckling C57BL/6 mice by inoculation of culture fluid of infected BAT-6 cell or human diploid cell or cerebrospinal fluid of patients intracerebrally and found demyelination of the pyramidal and the posterior tracts. Kitahara and Tagaya and Sakurada could not obtain meaningful results concerning neurovirulence of Inoue agent in suckling C57BL/6 mice. Since pallor of the pyramidal tract was observed in histological sections stained with luxol fast blue not only of the inoculated but also of uninoculated young mice, Inoue’s result is partly true, but it was considered by neuropathologists to illustrate a developmental stage of the myelin sheath, rather than an effect of virus infection.
The annual incidence of S.M.O.N. in Japan fell dramatically after the banning of sales of clioquinol from Sept. 8, 1970. The number of reported cases was 2418 in 1969, 1652 in 1970 (65 after September), 36 in 1971, 3 in 1972, 1 in 1973, and 0 in 1974. If the virus is shed at a high rate, as shown by Inoue, irrespective of stage of the illness, the chain of infection must continue and S.M.O.N. must arise as before. Our conclusion is that Inoue agent cannot be regarded as the etiological agent of S.M.O.N.
Kono’s letter offered a rare and necessary correction to a narrative shaped by fear and media hype rather than sound science. His emphasis on reproducibility, proper controls, and consistent epidemiological patterns stood in sharp contrast to Inoue’s speculative methods—serving as a cautionary reminder of the risks in declaring causation without solid evidence.
As Duesberg reported, the 1975 SMON Commission ultimately concluded that clioquinol was the likely cause. Their findings were supported by strong epidemiological data linking the drug to outbreaks, and by animal studies—particularly in dogs and cats—that reproduced SMON-like symptoms. Investigators also uncovered earlier case reports from countries such as Argentina, the UK, Sweden, and Australia, where similar neurological effects had been observed in patients taking clioquinol or related compounds. Many of these warnings had reached Ciba-Geigy, the drug’s manufacturer, years before the Japanese epidemic—a fact that later formed the basis for legal action.
On August 3, 1978, the Tokyo District Court formally ruled that the cause of SMON is clioquinol. Ciba-Geigy Japan and two domestic manufacturers issued an apology, stating: “Medical products manufactured and sold by us have been responsible for the occurrence of this tragedy in Japan—we extend our apologies.”
Despite this, Inoue persisted in his search for a “virus,” eventually renaming it the “Inoue-Melnick virus” to “avoid implicating them as causative agents of disease,” and conceding that it was no longer considered the “SMON virus.” In a 1984 paper, he admitted: “At the present state of knowledge, the virus has not been proven to be the causative agent of disease, hence its provisional designation as IMV.” He never succeeded in linking his “virus” to any disease.
The story that SMON research had ignored the evidence of a toxic cause for fifteen years and had sacrificed thousands of human lives to a flawed virus hypothesis is too embarrassing to the virus-hunting establishment to record.
-Peter Duesberg
The SMON episode is a striking example of how researchers can be misled by their own assumptions and the circular logic baked into their methods. Shigeyuki Inoue, operating under the government’s directive to find a “virus,” amassed a mountain of indirect evidence that, by virology’s own standards, “proved” a “viral” cause for SMON. He demonstrated cytopathic effects in cell cultures, documented “antibody” responses in animals and humans, identified “virus-like” particles under an electron microscope, and injected animals in artificial ways to produce symptoms that resembled the disease. Each of these methods, while routine in the virological playbook, rested on unproven premises and interpretation rather than direct, isolatable proof of a causative agent. Still, they were treated as if they constituted hard evidence.
Yet it was Reisaku Kono—a virologist himself—who interrupted this momentum. By stepping back from the virological echo chamber and comparing all available evidence without allegiance to a predetermined cause, he recognized that clioquinol—a widely prescribed pharmaceutical—offered a far more coherent and reproducible explanation for the SMON epidemic. Had Kono not insisted on a broader, more methodologically honest investigation, the “virus” would have been canonized as the cause, and clioquinol’s role likely buried in medical denialism.
The SMON fiasco laid bare the disturbing reality that toxic exposures, including iatrogenic ones, can be disguised as “infectious” disease when filtered through the dogma of virology. A polio-like condition was caused not by contagion, but by a drug given to relieve minor gastrointestinal discomfort—a drug promoted as a remedy that in truth helped drive the disease itself. This feedback loop, in which treatment perpetuates pathology, was only broken because someone dared to question the “virus-shaped” lens through which all illness was being viewed.
How many other illnesses—from polio to AIDS to “Covid-19”—rest on similar pillars of assumption, circular reasoning, and misdirection? How often are “viruses” blamed because doing so absolves the pharmaceutical industry, medical profession, and public health authorities of accountability? SMON is not just an embarrassing historical error—it is a warning. A warning that science ceases to be science when it becomes a tool for preserving consensus rather than discovering truth. The “virus” hypothesis, accepted on faith and propped up by indirect inference, serves as a convenient scapegoat—one that deflects from toxicological, environmental, and iatrogenic realities. The SMON deception deserves to be remembered, not as an anomaly, but as a blueprint for how the machinery of medical science can be hijacked by its own dogmas.
This essay should be required reading for all medical students and, yes, even virology students to at least impart a sense of humility and, can we hope, some healthy skepticism about received dogma. Brilliant work by Mr. Stone which will be dutifully ignored even by most "medical freedom" advocates. The virus paradigm controls the worldview of, well, the world. But the work of Mike Stone is a clarion call of hope.
How many S.M.O.N.'s are out there? I presented this matter to a know-nothing "health conscious" friend of mine, degree in physical therapy, total believer in "viruses." Her reaction: "Well, here they discovered something else. It's OK to assume a virus cause, because there are lots of viruses in the air." She, very counterculture-ish, WANTS to believe in viruses, because "Trump is evil and doesn't care about public health," and "It's intuitive, you're around sick people, and get sick, there must have been something transmitted from one to another." LOL,










This essay should be required reading for all medical students and, yes, even virology students to at least impart a sense of humility and, can we hope, some healthy skepticism about received dogma. Brilliant work by Mr. Stone which will be dutifully ignored even by most "medical freedom" advocates. The virus paradigm controls the worldview of, well, the world. But the work of Mike Stone is a clarion call of hope.
How many S.M.O.N.'s are out there? I presented this matter to a know-nothing "health conscious" friend of mine, degree in physical therapy, total believer in "viruses." Her reaction: "Well, here they discovered something else. It's OK to assume a virus cause, because there are lots of viruses in the air." She, very counterculture-ish, WANTS to believe in viruses, because "Trump is evil and doesn't care about public health," and "It's intuitive, you're around sick people, and get sick, there must have been something transmitted from one to another." LOL,