




As of May 11th, 2023, the “Covid” era officially comes to a close. The “virus” is no longer considered an emergency as, besides a few stray maskers, nearly everyone has gone away from “the new normal” and reverted back to the ways of “the old normal.” It is no longer necessary to lockdown and quarantine in the off chance that someones great aunt's second cousin, who tested positive, walked past a person while symptomless and possibly “infected” them, thus possibly “infecting” others by extension. There is no need to subject our nasal cavities to invasion by giant Q-tips regardless of the presence or absence of symptoms. It is no longer necessary to hide behind plastic shields that somehow stop the invisible “virus” from traveling up and around the square barrier. It is officially time to put away the social distancing stickers until the next “pandemic” holiday special is upon us and begin to walk freely amongst the living with the “normal” level of fear. The “pandemic” is over.
Hooray.
This official declaration is not so much of an ending as it is a calm before the storm. What this “ending” means is that they are putting away some of the measures that they have developed and utilized during this “pandemic,” such as stopping some of the surveillance programs as well as the free use of their products. What won't change is access to these rushed experimental and unapproved tests, drugs, and vaccines. While the “emergency” officially ends, somehow the FDA is still allowed to keep anything that they authorized by way of the EMERGENCY Use Authorization (EUA) to remain on the market, and even issue new ones, despite the lack of any emergency whatsoever. Thus, they technically never have to fully approve tests, drugs, and vaccines that were created during the “emergency” that were expedited without full approval and quality control. While these EUA products remain on the market, you may have to pay for these unapproved treatments out of your own pockets going forward, ensuring that the only major change occurring is that what was once free will now cost money. And just in case you thought that this was the “end of Covid,” they want you to know that “Covid” is still around, waiting and evolving to become a more severe threat that may require you to dust off the trusty mask and subject yourself to another booster in the future:
The U.S. COVID-19 public health emergency is ending. What does that mean?
“In January 2020, the U.S. government declared COVID-19 a public health emergency. Now, with coronavirus cases and deaths on the decline, that declaration is quickly approaching a predetermined expiration date.
Set to end on May 11, the public health emergency aimed to curb the coronavirus’ spread. In the pandemic’s earliest days, the declaration imposed temporary measures such as quarantines for people exposed to the virus (SN: 1/31/20). Later, it allowed federal officials to make tests, drugs and vaccines authorized by the U.S. Food and Drug Administration freely available to the public.
“Ending the public health emergency signals that we think we’ve turned a corner in what was a pretty dark time in America,” says health policy researcher Leighton Ku, who heads the Center for Health Policy Research at George Washington University in Washington, D.C. (It’s not the first pandemic-related declaration to end. On April 10, President Joe Biden signed legislation ending the national emergency, which had been issued in March 2020 to waive some requirements for federal health insurance programs, such as to allow coverage of telehealth visits.)
Even as the public health emergency becomes yet another relic of a traumatic period, COVID-19 isn’t going away. More than 1,000 people in the United States died from COVID-19 from April 20 to April 26, according to the U.S. Centers for Disease Control and Prevention. And the coronavirus continues to evolve. Although not all new variants are worrisome, some can be (SN: 10/17/22). So it remains to be seen whether now is the time to let our guard down, Ku says.
Tests, drugs and vaccines will remain important tools to control the virus’ spread, and researchers hope to improve our arsenal.”
Millions of people may lose access to free testing
“COVID tests — at-home and lab versions — that were authorized by the FDA over the last three years will remain available. These tests were granted emergency use authorizations, or EUAs, which allow public access to tests that are not formally approved by the FDA. Instead of expiring with the public health emergency, the FDA can decide when it wants to end individual EUAs, and it can still issue EUAs for any new tests that might be developed.
What may change is who pays for tests and diagnostics. It all comes down to insurance.”
Availability of COVID vaccines and treatments won’t change (for now)
“The end of the national emergency did not impact people’s ability to access vaccines and antiviral treatments. Nor will the end of the public health emergency.
Vaccines and treatments will “generally not be affected,” the U.S. Department of Health and Human Service, or HHS, says. The FDA can also continue issuing EUAs for any new vaccines or treatments that might be developed to fight future variants.
However another big shift looms later this year. Throughout the pandemic, the U.S. government stockpiled vaccines and treatments to fight COVID-19 and provided them to the public for free. Congress has decided not to continue funding these efforts.”
Research into new COVID vaccines and treatments will continue
“The bulk of the funding for coronavirus research wasn’t tied directly to the public health emergency, so ongoing and future studies won’t come to a halt. What will change is how some data get reported to the CDC.
While most CDC data tracking isn’t directly affected by the public health emergency’s end, daily reports of COVID-related hospitalizations may come less frequently, according to the agency. Labs will also no longer be required to report COVID-19 lab test results, making it harder to figure out what percentage of tests are positive — a metric that’s useful for monitoring new surges of infections. Reports of increasing cases and hospitalizations may be slightly delayed for places that don’t regularly release the information to the CDC, potentially making it more difficult for people to know exactly when cases start rising in their community and it’s time to start wearing masks again.”
What one must realize is that it was always known that the implemented “Covid” measures such as lockdowns, quarantines, mass testing, surveillance tracking, social distancing, masking, etc. were never going to last indefinitely. These measures were implemented under the guise of a threat so that these restrictions and invasions, that would have normally been challenged by the majority in the past, were easily accepted and allowed due to the fear of the invisible “threat.” They have now become an annoying but accepted strategy by the public at large to deal with any future “viral” outbreaks. These measures are being incorporated into future response plans, as stated by the CDC:
End of Public Health Emergency
“The United States has mobilized and sustained a historic response to the COVID-19 pandemic. As a nation, we now find ourselves at a different point in the pandemic – with more tools and resources than ever before to better protect ourselves and our communities.
CDC has been working for many months to fold the agency’s COVID-19 emergency response activities into its existing structure and programs, as part of an ongoing transition to sustainable public health practice. The agency has also been working with partners, including states and local territories, to prepare for the end of the PHE declaration and communicate updated reporting requirements and cadences.”
https://www.cdc.gov/coronavirus/2019-ncov/your-health/end-of-phe.html
This is an obvious example of what is known as the Hegelian dialectic, where a problem is presented (“SARS-COV-2"), the reaction occurs (fear of the “virus”), and the solution is dispensed to the public (“Covid” measures and restrictions). These measures are now accepted as a part of the “new normal” solution that can be utilized whenever desired. If a “bigger threat” arrives, this game of push and pull for harsher methods can begin anew, and it will most definitely begin anew if the words of the officials running the WHO are to be believed. Even though the WHO officially ended their own “public health emergency” on May 5th, 2023, the organization laid out the plans for the franchise going forward by stating:
There is still a public health threat
The “virus” continues to evolve and is here to stay
One pandemic will not end until the next one begins
The emergency declaration can be re-enacted at any moment
The scars must serve as a permanent reminder of the upcoming threats
WHO says Covid-19 is no longer a global health emergency
“There’s still a public health threat out there, and we all see that every day in terms of the evolution of this virus, in terms of its global presence, its continued evolution and continued vulnerabilities in our communities, both societal vulnerabilities, age vulnerabilities, protection vulnerabilities, and many other things,” said Dr. Mike Ryan, executive director of WHO’s Health Emergencies Programme.
“So, we fully expect that this virus will continue to transmit, but this is the history of pandemics,” Ryan said. “In most cases, pandemics truly end when the next pandemic begins. I know that’s a terrible thought but that is the history of pandemics.”
“Dr. Maria Van Kerkhove, WHO’s Covid-19 technical lead and head of its program on emerging disease, said that the emergency phase of the Covid-19 crisis is over but the disease is “here to stay” and the coronavirus that causes the disease is not going away any time soon.”
“While we’re not in the crisis mode, we can’t let our guard down,” Van Kerkhove said. “Epidemiologically, this virus will continue to cause waves. What we are hopeful of is that we have the tools in place to ensure that the future waves do not result in more severe disease, don’t result in waves of death and we can do that with the tools we have at hand. We just need to make sure that we are tracking the virus because it will continue to evolve.”
“Tedros said that, if needed, he would not hesitate to convene another emergency committee meeting and declare a global health emergency again if there is a significant rise in Covid-19 cases or deaths in the future.
“Covid-19 has left and continues to leave deep scars on our world. Those scars must serve as a permanent reminder of the potential for new viruses to emerge with devastating consequences,” Tedros said.”
Thus, while those who were unaware of the fraud that has been perpetrated on humanity for the past three years may be celebrating this “ending,” many of us have been aware of the plot from the beginning and have been planning for the inevitable sequel while looking for ways to cancel the franchise before the next release date.
In the spirit of actually ending this madness once and for all, I am extremely excited to announce a very exciting project that I have been a part of for the last few months. From the brilliant mind of The Way Forward's Alec Zeck comes “The End of Covid,” an 88 part virtual summit covering every topic that one can imagine regarding germ theory and the fraud of virology. This gigantic undertaking begins June 20th, involving a plethora of amazing individuals who have been working hard to spread the message that there is nothing to fear. Many names will be recognizable such as Dr. Tom Cowan, Dr. Andrew Kaufman, Drs. Sam and Mark Bailey, Dr. Amandha Vollmer, Dr. Kelly Brogan, etc. However, there are many equally important lesser known as well as new and exciting voices lending their support, input, and expertise to this event.
Personally, I have been involved in some fascinating discussions that have been very rewarding. Whether it was examining the scientific method and logical fallacies with Dr. Jordan Grant, covering theoretical antibodies with Mike Donio and Dr. Stefano Scoglio, or exploring the history of virology with Steve Falconer and Dr. Mark Bailey, it has been a truly fantastic experience. It is a labor of love by concerned individuals who are interested in ending this fraudulent paradigm and, in doing so, changing this world for the better for future generations to come. I hope that you all get the chance to check it out and enjoy, learn from, and grow from this experience.
Let's share this far and wide so that we can get as many eyes on this extremely important information as soon as possible in order to ensure that any planned sequels are cancelled. To stay informed on “The End of Covid,” please visit theendofcovid.com.
Now, in keeping with the theme of closing the curtain on “Covid,” let's re-examine the core elements as to why there was never any reason for the curtains to open in order to spread the fear of “SARS-COV-2” in the first place. While the information presented here is in reference to “SARS-COV-2” specifically, it can apply to all of these invisible “pathogens” as well.
1. There is no new disease.
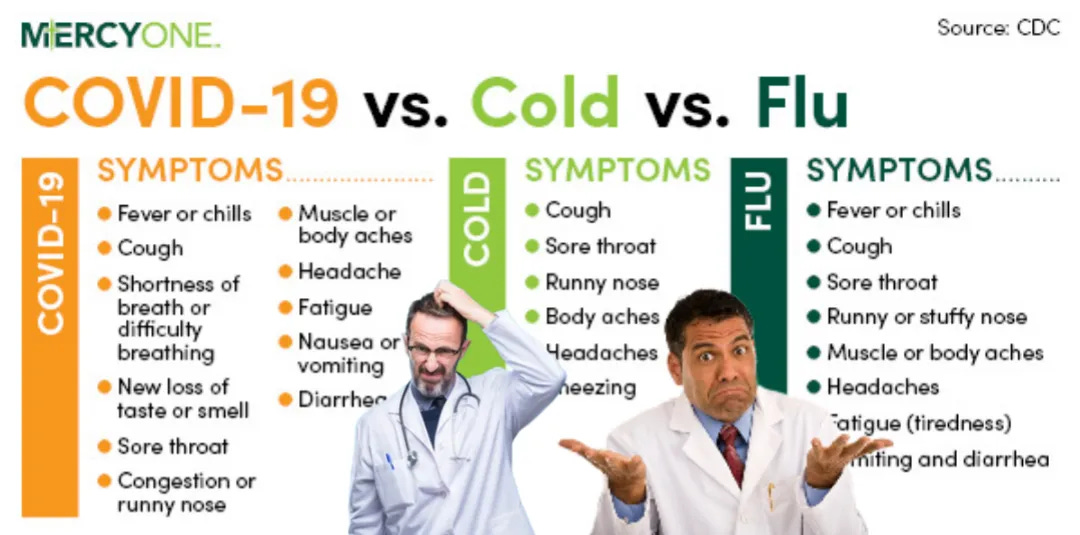
To begin with, people seem to not realize that there are absolutely no new or specific symptoms that define “Covid-19.” The exact same symptoms of disease that we see with the flu and any other respiratory disease were given a new name. It truly is as simple as that. Don't believe me? There are numerous sources claiming that there is no way to differentiate “Covid-19” from any other respiratory disease based on clinical signs, symptoms, and laboratory results. According to the CDC:
“You cannot tell the difference between flu and COVID-19 by symptoms alone because some of the symptoms are the same.”
https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/clinical-considerations-diagnosis.html
It was known as early as March 2020 that the symptoms associated with “Covid” were non-specific and overlapped with other respiratory diseases:
Diagnosing COVID-19: The Disease and Tools for Detection
“The symptoms expressed by COVID-19 patients are nonspecific and cannot be used for an accurate diagnosis. Guan et al. reported that 44% of 1099 COVID-19 patients from China had a fever when they entered the hospital and that 89% developed a fever while in hospital.25 They further found that patients had a cough (68%), fatigue (38%), sputum production (34%), and shortness of breath (19%). Many of these symptoms could be associated with other respiratory infections.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7144809/
A September 2021 study admitted that there is absolutely no reliable clinical or laboratory parameters to distinguish safely between “Covid-19” and airway infections of other origins:
What about the others: differential diagnosis of COVID-19 in a German emergency department
“For many common ED diagnoses, COVID-19 should be considered a differential diagnosis. COVID-19 cannot be distinguished from COVID-19 negative respiratory infections by clinical signs, symptoms, or laboratory results. When hospitalization is necessary, the clinical course of COVID-19 airway infections seems to be more severe compared to other respiratory infections.”
Discussion
“Early triage and differential diagnosis of patients presenting with typical clinical symptoms of COVID-19 remain very challenging but relevant. Our study had the following main findings:
Differential diagnosis of typical COVID-19 symptoms is very broad and comprises many common respiratory, infectious, and cardiovascular diseases, whereas respiratory diseases are the most frequent. Diseases from nearly every field of clinical medicine can mimic a clinical picture like that of COVID-19, with respiratory diseases being the most prevalent. Older patients may be even more challenging since the clinical picture may be atypical with syncope and malaise [12].
Patients with COVID-19 present with similar symptoms as COVID-19 negative respiratory infections, so clinical discrimination is not reliable.”
Conclusions
“Differential diagnoses of COVID-19 are plentiful and comprise many common diseases, most notably ailments associated with respiratory impairment. Triage remains challenging in the emergency department since there are no reliable clinical or laboratory parameters to distinguish safely between COVID-19 and airway infections of other origins. When inpatient, COVID-19 takes a more severe clinical course than comparable COVID-19 negative airway infections. Therefore, a strict isolation policy together with broad and rapid testing will remain the most important measures for the months to come.”
https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-021-06663-x
Remember the ground glass opacities that were the sign of the terrifying new disease necessitating chest scans as a form of diagnosis?
A new coronavirus associated with human respiratory disease in China
“On the first day of admission (day 6 after the onset of disease), chest radiographs were abnormal with air-space shadowing such as ground-glass opacities, focal consolidation and patchy consolidation in both lungs (Extended Data Fig. Fig.1).1).”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7094943/
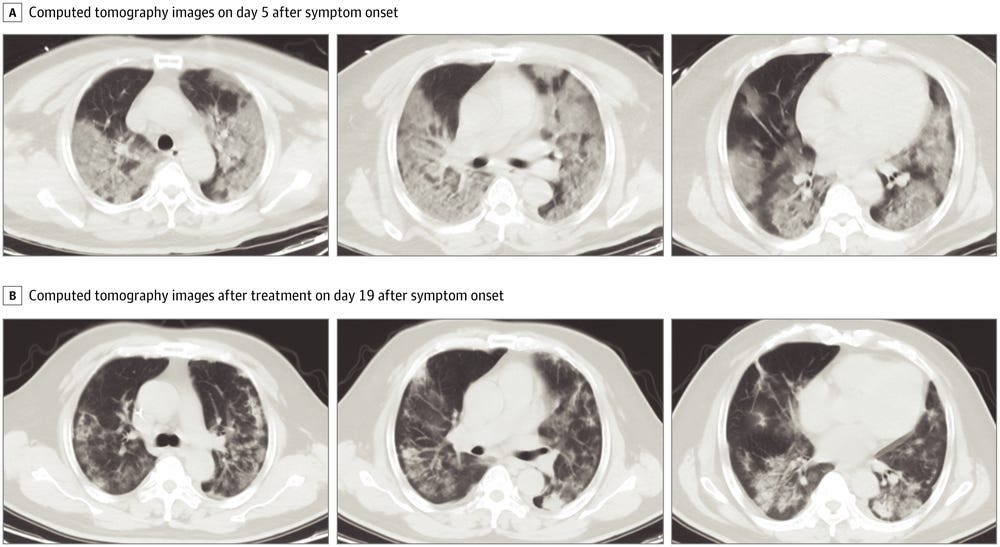
Finding this ground glass opacity in patients via CT scans was said to be an indicator of severe “Covid” disease. It was one of the early defining characteristics. However, this “terrifying” finding, which was spread throughout the media in order to sell the public on the new threat, is not specific to “Covid” at all and is found in many conditions, including in those who vape:
Many coronavirus patients have 'ground glass' in their lung scans. Here's what that looks like.
“Patients with severe cases typically develop fluid in their lungs, similar to those seen in standard pneumonia cases. That fluid can be detected on a CT scan, where it shows up in the form of white patches that doctors call "ground glass."
CT scans are considered less thorough than lab tests, but here's what physicians look for to detect the coronavirus in a scan.”
“On its own, Lakhani said, ground glass isn't particularly helpful for identifying a coronavirus.
"You can see it with all types of infections — bacterial, viral, or sometimes even non-infectious causes," Lakhani said. "Even vaping could sometimes appear this way."
It was known that using CT scans as a method of detection was non-specific and that it did not even match up with PCR results. In other words, there were cases of those who had the ground glass opacities while testing negative via PCR and those who did not have the finding and still tested positive for “Covid” via PCR:
Review of the Chest CT Differential Diagnosis of Ground-Glass Opacities in the COVID Era
“The purpose of this review is to discuss and differentiate typical imaging findings of COVID-19 from those of other diseases, which can appear similar in the first instance. The typical CT findings of COVID-19 are bilateral and peripheral predominant ground-glass opacities. As per the Fleischner Society consensus statement, CT is appropriate in certain scenarios, including for patients who are at risk for and/or develop clinical worsening. The probability that CT findings represent COVID-19, however, depends largely on the pretest probability of infection, which is in turn defined by community prevalence of infection. When the community prevalence of COVID-19 is low, a large gap exists between positive predictive values of chest CT versus those of reverse transcriptase polymerase chain reaction. This implies that with use of chest CT there are a large number of false-positive results. Imaging differentiation is important for management and isolation purposes and for appropriate disposition of patients with false-positive CT findings.”
https://pubs.rsna.org/doi/full/10.1148/radiol.2020202504
They even mention that the accuracy of a CT scan finding depends upon community prevalence of the disease, which is a factor that also affects PCR results. When disease prevalence is low, false-positives are high. However, in order to determine disease prevalence, the disease must be able to be diagnosed clinically in order to determine cases. However, “Covid” can not be diagnosed clinically as there are no new or specific symptoms. Even the dreaded loss of taste and smell, often hyped as a specific symptom of “Covid,” was always a known factor in other diseases:
Doctors warn an inability to smell could be a symptom of Covid-19 — but caution the evidence is preliminary
“There are a number of unanswered questions about the new potential symptom, which at this point, is thought to be temporary. Experts aren’t sure how common it is, or at what point in the progression of the disease a patient loses the ability to smell. They also want to be sure the new symptom isn’t merely a sign of allergies, a cold, or the seasonal flu, all of which can lead a person to develop anosmia or ageusia, the reduced sense of taste that can sometimes accompany an inability to smell.”
https://www.statnews.com/2020/03/23/coronavirus-sense-of-smell-anosmia/
As there are no new symptoms of disease, there is no new disease. The “Covid” hoax was nothing but a rebranding, repackaging, and reselling of the same symptoms as something frightening and new. Marketing 101. Without any new or specific signs and symptoms, “Covid” can not be diagnosed clinically. If “Covid” can not be diagnosed clinically, then the tests used as diagnostic tools can not be accurate. See the problem yet?
2. There is no “SARS-COV-2.”

A common mistake the vast majority of people make is trusting that the evidence presented to them is accurate and valid without ever investigating whether this assumption is true or not. They believe that if a paper is peer-reviewed and published in a scientific journal and/or reported on by the mainstream media, the information must indeed be true. However, this is, more often than not, not the case, and in regard to “SARS-COV-2,” the evidence offered was neither scientific nor actual proof of the existence of a “novel pathogen” capable of causing the non-specific symptoms of disease associated with it.
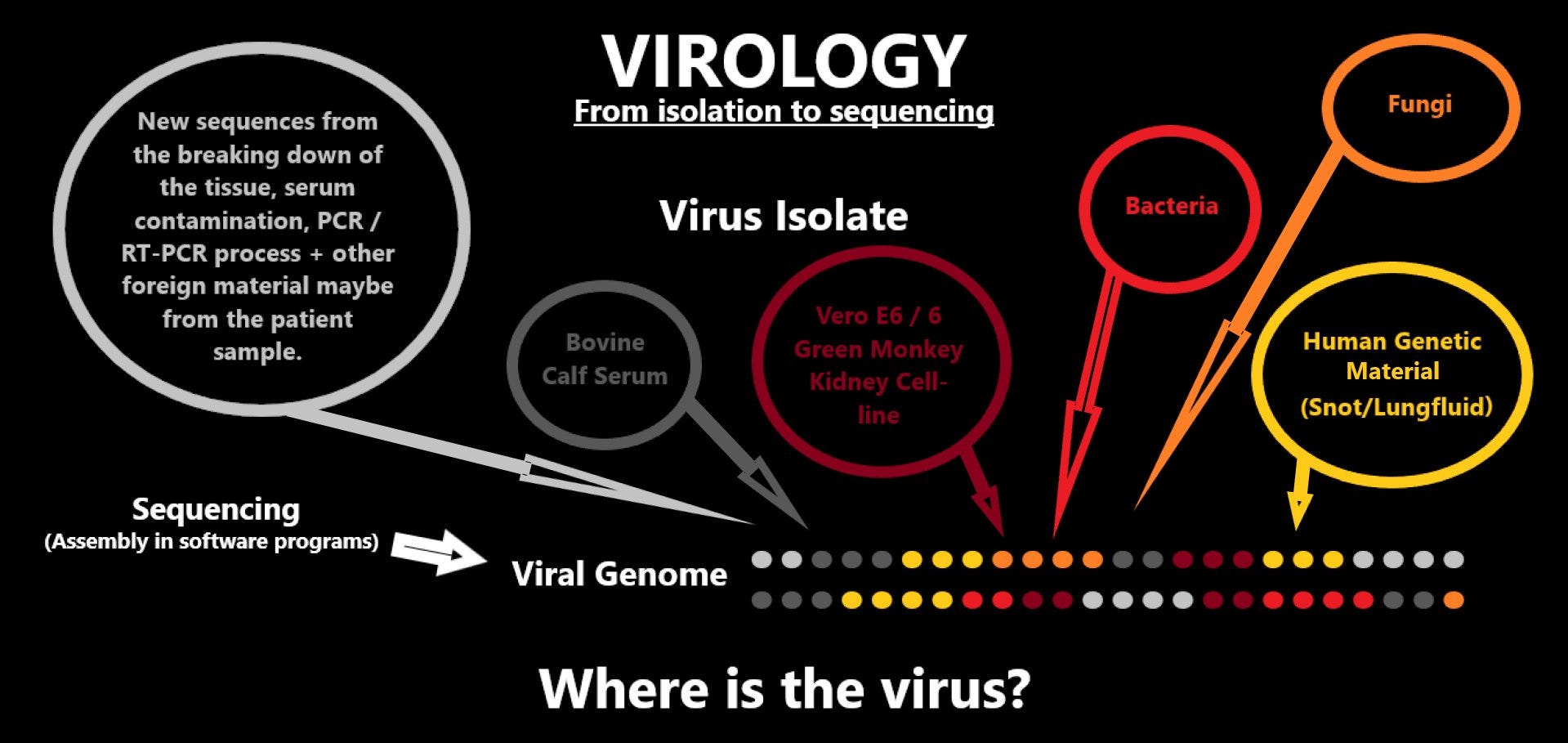
To begin with, the genome for the “virus” in question was nothing but an in silico (in the computer) creation stemming from the bronchoalveolar lavage fluid (BALF) taken from the lungs of a single patient. No proper scientific controls, such as using fluids from healthy hosts or diseased hosts said to be suffering from other causes, were used in order to rule out that the genome only came from those who were considered “SARS-COV-2” cases. The sample used for sequencing was unpurified, meaning that they did not put it through any purification procedures such as ultracentrifugation in order to remove any host or foreign materials, contaminants, pollutants, etc., leaving only the assumed “viral” particles to sequence from. This is a problem as there is a high amount of off-target RNA/DNA, even if purification steps are performed, that will get sequenced as well, as admitted by the WHO:
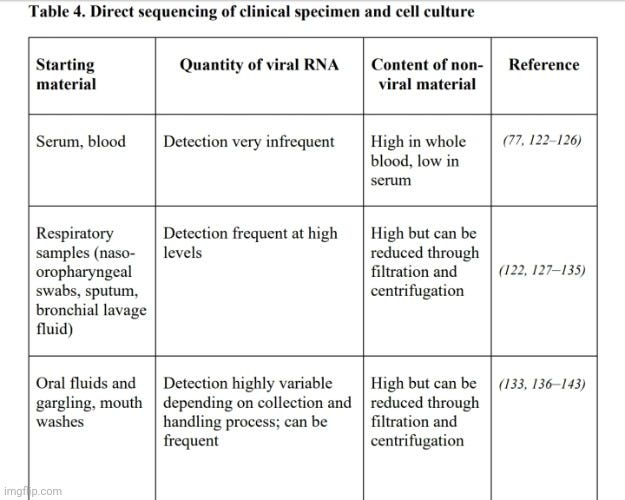
Genomic sequencing of SARS-CoV-2
“Depletion of host or other non-SARS-CoV-2 genetic material in a sample leads to a higher proportion of SARS-CoV-2 reads in generated sequence data and therefore a higher chance of recovering a full genome. SARS-CoV-2 metagenomic approaches therefore typically include steps to remove host and bacterial cells, through either centrifugation or filtration prior to RNA extraction, or chemical or enzymatic removal of unwanted DNA/RNA. This is easier for liquid samples, from which cells can be more easily separated, such as bronchoalveolar lavage (Table
4). Ribosomal RNA (rRNA) and DNA content are also commonly depleted during library preparation for virus RNA sequencing, and carrier RNA is often omitted from extractions or replaced with linear polyacrylamide. Despite such measures, samples may still contain high quantities of off-target host DNA/RNA that may also be sequenced. Metagenomic approaches therefore generally benefit from input of samples with high virus loads (such that a reasonable proportion of the genetic material in the sample is virus).”“Metagenomic sequencing typically produces high numbers of off-target, non-virus reads. It is also often (though not always, depending on the sequencing platform and multiplexing) more costly than targeted capture-based or amplicon-based sequencing approaches, because more data have to be produced to generate one SARS-CoV-2 genome. Moreover, pretreatment steps that are particularly beneficial for metagenomics, such as centrifugation, are not typically performed for molecular diagnostic assays so new extractions that incorporate pretreatment steps may have to be performed for metagenomic sequencing.”
To create the “SARS-COV-2” genome, Fan Wu et al. performed metagenomic sequencing on the entire sample without any purification steps and then assembled the resulting RNA fragments into a theoretical genome of “SARS-COV-2” by referencing genomes of other “coronaviruses” that were also created from unpurified samples. Thus, they generated and used random short fragments of unknown provenance with no evidence that these fragments ever came from a single source, and then matched it to other “viral” genomes with no evidence that any of the fragments were ever “viral:”
A new coronavirus associated with human respiratory disease in China
“To investigate the possible aetiological agents associated with this disease, we collected bronchoalveolar lavage fluid (BALF) and performed deep meta-transcriptomic sequencing. The clinical specimen was handled in a biosafety level 3 laboratory at Shanghai Public Health Clinical Center. Total RNA was extracted from 200 μl of BALF and a meta-transcriptomic library was constructed for pair-end (150-bp reads) sequencing using an Illumina MiniSeq as previously described4,6,7,8. In total, we generated 56,565,928 sequence reads that were de novo-assembled and screened for potential aetiological agents. Of the 384,096 contigs assembled by Megahit9, the longest (30,474 nucleotides (nt)) had a high abundance and was closely related to a bat SARS-like coronavirus (CoV) isolate—bat SL-CoVZC45 (GenBank accession number MG772933)—that had previously been sampled in China, with a nucleotide identity of 89.1% (Supplementary Tables 1, 2). The genome sequence of this virus, as well as its termini, were determined and confirmed by reverse-transcription PCR (RT–PCR)10 and 5′/3′ rapid amplification of cDNA ends (RACE), respectively. This virus strain was designated as WH-Human 1 coronavirus (WHCV) (and has also been referred to as ‘2019-nCoV’) and its whole genome sequence (29,903 nt) has been assigned GenBank accession number MN908947. Remapping the RNA-sequencing data to the complete genome of WHCV resulted in an assembly of 123,613 reads, providing 99.99% genome coverage at a mean depth of 6.04× (range, 0.01–78.84×) (Extended Data Fig. 3). The viral load in the BALF sample was estimated by qPCR to be 3.95 × 108 copies per ml (Extended Data Fig. 4).
The viral genome organization of WHCV was determined by sequence alignment to two representative members of the genus Betacoronavirus: a coronavirus associated with humans (SARS-CoV Tor2, GenBank accession number AY274119) and a coronavirus associated with bats (bat SL-CoVZC45, GenBank accession number MG772933). The un-translational regions and open-reading frame (ORF) of WHCV were mapped on the basis of this sequence alignment and ORF prediction. The WHCV viral genome was similar to these two coronaviruses (Fig. 1 and Supplementary Table 3). The order of genes (5′ to 3′) was as follows: replicase ORF1ab, spike (S), envelope (E), membrane (M) and nucleocapsid (N). WHCV has 5′ and 3′ terminal sequences that are typical of betacoronaviruses, with 265 nt at the 5′ terminal end and 229 nt at the 3′ terminal end. The predicted replicase ORF1ab gene of WHCV is 21,291 nt in length and contained 16 predicted non-structural proteins (Supplementary Table 4), followed by (at least) 13 downstream ORFs. Additionally, WHCV shares a highly conserved domain (LLRKNGNKG: amino acids 122–130) in nsp1 with SARS-CoV. The predicted S, ORF3a, E, M and N genes of WHCV are 3,822, 828, 228, 669 and 1,260 nt in length, respectively. In addition to these ORF regions, which are shared by all members of the subgenus Sarbecovirus, WHCV is similar to SARS-CoV in that it carries a predicted ORF8 gene (with a length of 366 nt) that is located between the M and N ORF genes. The functions of WHCV ORFs were predicted on the basis of those of known coronaviruses and are described in Supplementary Table 5.”
“These genomic and clinical similarities to SARS, as well as its high abundance in clinical samples, provides evidence for an association between WHCV and the ongoing outbreak of respiratory disease in Wuhan and across the world. Although the isolation of the virus from only a single patient is not sufficient to conclude that it caused these respiratory symptoms, our findings have been independently corroborated in further patients in a separate study29.”
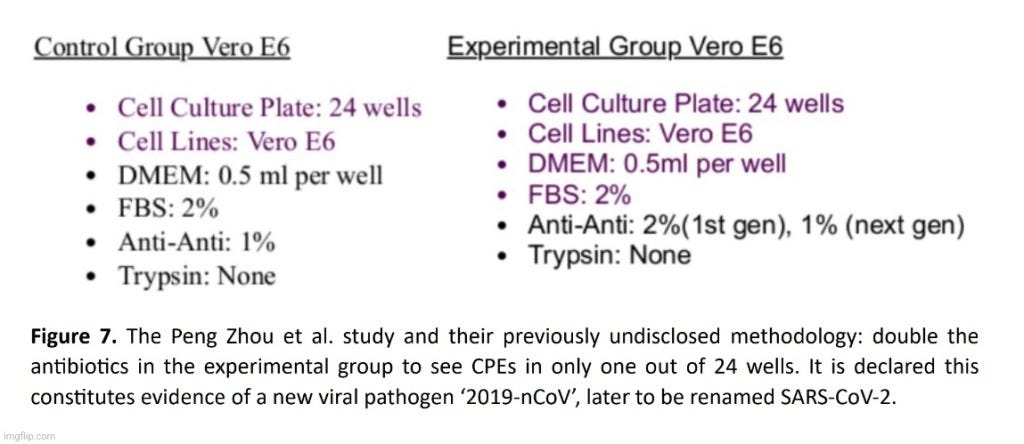
If you noticed in the last paragraph highlighted, Wu et al. admitted that their finding of a genome from a single patient was not enough in order to claim that their in silico creation was the cause of the symptoms associated with it. Thus, they relied upon a separate study by Zhou et al. as confirmation. However, there are a few problems in doing so. For starters, the researchers did not perform any purification steps and cultured their BALF sample from a single patient in Vero (African green monkey kidney) and Huh7 (male hematoma cancer) cells mixed with numerous additives such as antibiotics, antifungals, baby cow blood, trypsin, etc. This process is the exact opposite of purification and isolation. Zhou et al. also did not perform proper scientific controls using the fluids of a healthy host or a sick host said to be suffering from a different cause during their sequencing and cell culture experiments. In fact, Zhou et al. did not even treat the mock infected cultures that they performed the same as the experimental group, minus the independent variable (which they never have). Instead, they doubled the dose of the toxic antibiotics used in the experimental group, thus nullifying the data from the controls.
On top of that, Zhou et al. admitted that they did not satisfy Koch's Postulates, the four logical steps that must be satisfied in order to claim a microbe is the causative agent of disease. Zhou et al. performed no pathogenicity studies in order to prove a causal relationship between their cell cultured creation and the non-specific symptoms of disease associated with it:
A pneumonia outbreak associated with a new coronavirus of probable bat origin
“The study provides a detailed report on 2019-nCoV, the likely aetiological agent responsible for the ongoing epidemic of acute respiratory syndrome in China and other countries. Virus-specific nucleotide-positive and viral-protein seroconversion was observed in all patients tested and provides evidence of an association between the disease and the presence of this virus. However, there are still many urgent questions that remain to be answered. The association between 2019-nCoV and the disease has not been verified by animal experiments to fulfil the Koch’s postulates to establish a causative relationship between a microorganism and a disease. We do not yet know the transmission routine of this virus among hosts.”
Another major paper used in the early months of 2020 as proof for the existence of “SARS-COV-2” and its supposed role in the not-so-new “Covid” disease by Zhu et al. also admitted to not satisfying Koch's Postulates. None of the researchers attempted to prove a causal role for the random A,C,T,G's in a computer database with the disease it was associated with:
A Novel Coronavirus from Patients with Pneumonia in China, 2019
Although our study does not fulfill Koch’s postulates, our analyses provide evidence implicating 2019-nCoV in the Wuhan outbreak. Additional evidence to confirm the etiologic significance of 2019-nCoV in the Wuhan outbreak include identification of a 2019-nCoV antigen in the lung tissue of patients by immunohistochemical analysis, detection of IgM and IgG antiviral antibodies in the serum samples from a patient at two time points to demonstrate seroconversion, and animal (monkey) experiments to provide evidence of pathogenicity.”
https://www.nejm.org/doi/full/10.1056/nejmoa2001017
Even more concerning is that none of the electron microscope images of the so-called “virus” used to whip people into a frenzy ever came directly from the fluids of a sick patient. These particles picked out as the representative only ever come from unpurified cell culture supernatants. This was admitted by Zhu et al. and other researchers:
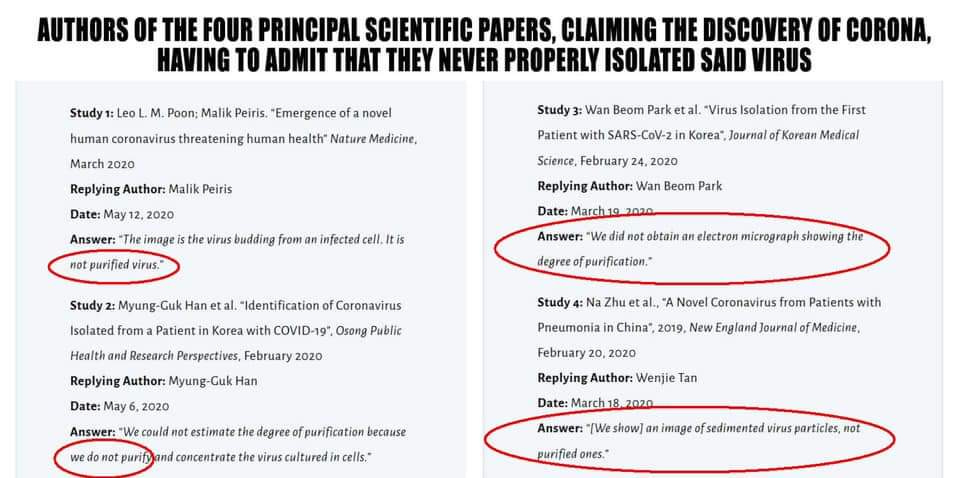
Thus, there is no evidence that the particles, picked out from an unpurified mess of similar and/or identical particles, even belong to the theoretical genome conjured up by Fan Wu et al. in the first place.

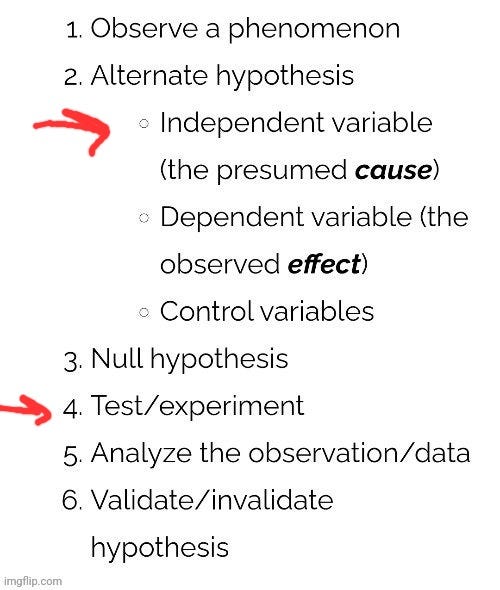
What we are left with is one pseudoscientific mess as, at no point in time, did any of these researchers have a valid independent variable in purified and isolated particles that they proved that the genome and EM images came from and actually caused the disease it was associated with. Instead, we have experiments being performed with no independent variable whatsoever, which goes against the scientific method. The independent variable (i.e. the assumed “viral” particles) must exist before the cell culture experiment and any sequencing is done. What we have is pseudoscientific evidence paraded around as if it were scientific.
3. There was no “viral” pandemic.

There are many reasons why there was never any “pandemic” and far too many to cover here. However, with no new disease and no scientific evidence of any “virus,” it should be clear that there was no “viral” pandemic. What we had, instead, was a testing pandemic based upon fraudulent techniques that should have never been used for diagnosis in the first place. As stated earlier, it is admitted that in order for any PCR result to be accurate, disease prevalence must be known. If it is not known, then the rate of false-positives is high. In order to determine disease prevalence, the cases must be known, as seen in this CDC graphic:
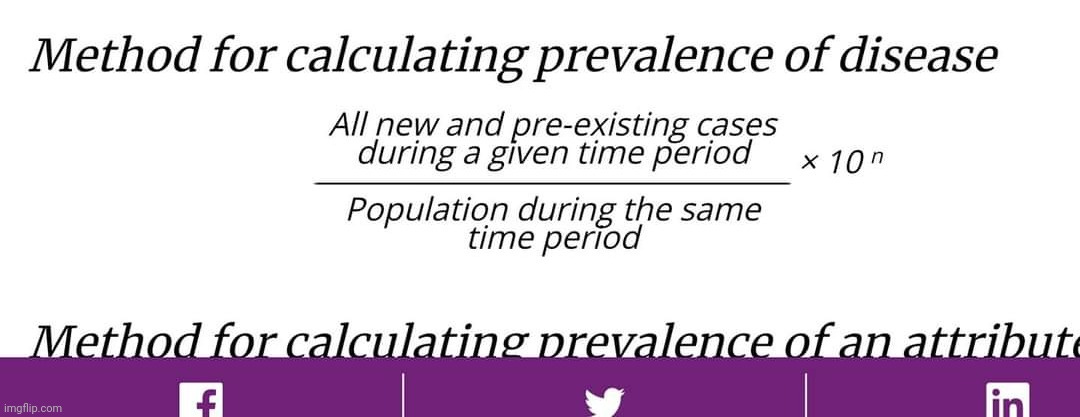
Cases can only be determined by clinical diagnosis. Yet as we discussed earlier, this is impossible as there are no new or specific symptoms that define “Covid” as it overlaps with respiratory and other diseases. Thus, there is no ability to determine cases in order to figure out disease prevalence so that an “accurate” PCR result is obtained. Thus, all cases generated by PCR, the “gold standard,” are inaccurate and what we ended up with was nothing more than a pandemic of false-positives. This same scenario was witnessed on a smaller scale in 2007 with a supposed whooping cough outbreak at the Dartmouth Medical Center. Long story short, every single positive case detected by PCR turned out to be false-positive when they could not grow the Bordetella pertussis bacterium in culture, even though the symptoms were 100% consistent with whooping cough. It was decided that those who were ill must have been suffering from some other respiratory disease. I am providing highlights but the whole article is definitely worth a read in order to understand that PCR can be easily used to create a “pandemic” that never was:
Faith in Quick Test Leads to Epidemic That Wasn’t
“Dr. Brooke Herndon, an internist at Dartmouth-Hitchcock Medical Center, could not stop coughing. For two weeks starting in mid-April last year, she coughed, seemingly nonstop, followed by another week when she coughed sporadically, annoying, she said, everyone who worked with her.
Before long, Dr. Kathryn Kirkland, an infectious disease specialist at Dartmouth, had a chilling thought: Could she be seeing the start of a whooping cough epidemic? By late April, other health care workers at the hospital were coughing, and severe, intractable coughing is a whooping cough hallmark. And if it was whooping cough, the epidemic had to be contained immediately because the disease could be deadly to babies in the hospital and could lead to pneumonia in the frail and vulnerable adult patients there.
It was the start of a bizarre episode at the medical center: the story of the epidemic that wasn’t.
For months, nearly everyone involved thought the medical center had had a huge whooping cough outbreak, with extensive ramifications. Nearly 1,000 health care workers at the hospital in Lebanon, N.H., were given a preliminary test and furloughed from work until their results were in; 142 people, including Dr. Herndon, were told they appeared to have the disease; and thousands were given antibiotics and a vaccine for protection. Hospital beds were taken out of commission, including some in intensive care.
Then, about eight months later, health care workers were dumbfounded to receive an e-mail message from the hospital administration informing them that the whole thing was a false alarm.
Not a single case of whooping cough was confirmed with the definitive test, growing the bacterium, Bordetella pertussis, in the laboratory. Instead, it appears the health care workers probably were afflicted with ordinary respiratory diseases like the common cold.
Now, as they look back on the episode, epidemiologists and infectious disease specialists say the problem was that they placed too much faith in a quick and highly sensitive molecular test that led them astray.
Infectious disease experts say such tests are coming into increasing use and may be the only way to get a quick answer in diagnosing diseases like whooping cough, Legionnaire’s, bird flu, tuberculosis and SARS, and deciding whether an epidemic is under way.”
“Many of the new molecular tests are quick but technically demanding, and each laboratory may do them in its own way. These tests, called “home brews,” are not commercially available, and there are no good estimates of their error rates. But their very sensitivity makes false positives likely, and when hundreds or thousands of people are tested, as occurred at Dartmouth, false positives can make it seem like there is an epidemic.”
“At Dartmouth the decision was to use a test, P.C.R., for polymerase chain reaction. It is a molecular test that, until recently, was confined to molecular biology laboratories.
“That’s kind of what’s happening,” said Dr. Kathryn Edwards, an infectious disease specialist and professor of pediatrics at Vanderbilt University. “That’s the reality out there. We are trying to figure out how to use methods that have been the purview of bench scientists.”
The Dartmouth whooping cough story shows what can ensue.”
“Yet, epidemiologists say, one of the most troubling aspects of the pseudo-epidemic is that all the decisions seemed so sensible at the time.”
“That was the first problem in deciding whether there was an epidemic at Dartmouth.
The second was with P.C.R., the quick test to diagnose the disease, Dr. Kretsinger said.
With pertussis, she said, “there are probably 100 different P.C.R. protocols and methods being used throughout the country,” and it is unclear how often any of them are accurate. “We have had a number of outbreaks where we believe that despite the presence of P.C.R.-positive results, the disease was not pertussis,” Dr. Kretsinger added.
At Dartmouth, when the first suspect pertussis cases emerged and the P.C.R. test showed pertussis, doctors believed it. The results seem completely consistent with the patients’ symptoms.
“That’s how the whole thing got started,” Dr. Kirkland said. Then the doctors decided to test people who did not have severe coughing.
“Because we had cases we thought were pertussis and because we had vulnerable patients at the hospital, we lowered our threshold,” she said. Anyone who had a cough got a P.C.R. test, and so did anyone with a runny nose who worked with high-risk patients like infants.
“That’s how we ended up with 134 suspect cases,” Dr. Kirkland said. And that, she added, was why 1,445 health care workers ended up taking antibiotics and 4,524 health care workers at the hospital, or 72 percent of all the health care workers there, were immunized against whooping cough in a matter of days.
“If we had stopped there, I think we all would have agreed that we had had an outbreak of pertussis and that we had controlled it,” Dr. Kirkland said.”
“Dr. Cathy A. Petti, an infectious disease specialist at the University of Utah, said the story had one clear lesson.
“The big message is that every lab is vulnerable to having false positives,” Dr. Petti said. “No single test result is absolute and that is even more important with a test result based on P.C.R.”
https://web.archive.org/web/20200713060324/https://www.nytimes.com/2007/01/22/health/22whoop.html
In addition to the fact that all PCR cases are false-positives due to the lack of a definable new disease able to be diagnosed clinically, the PCR tests themselves were never calibrated nor validated to purified and isolated “virus.” In fact, the very first PCR test created for the “pandemic” was developed by Christian Drosten entirely in a computer based off of social media reports with no “virus” available:
Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR
“In the present case of 2019-nCoV, virus isolates or samples from infected patients have so far not become available to the international public health community. We report here on the establishment and validation of a diagnostic workflow for 2019-nCoV screening and specific confirmation, designed in absence of available virus isolates or original patient specimens. Design and validation were enabled by the close genetic relatedness to the 2003 SARS-CoV, and aided by the use of synthetic nucleic acid technology.”
“Before public release of virus sequences from cases of 2019-nCoV, we relied on social media reports announcing detection of a SARS-like virus. We thus assumed that a SARS-related CoV is involved in the outbreak. We downloaded all complete and partial (if > 400 nt) SARS-related virus sequences available in GenBank by 1 January 2020.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6988269/#!po=0.746269
The Drosten test was the main one utilized around the world. There were many problems with the test that were outlined in the Corman-Drosten review by a team of independent scientists and researchers. The Drosten paper itself was peer-reviewed and accepted within 24 hours, which is virtually unheard of. Meanwhile, the CDC's own PCR test used in the US was also developed without any “virus” available:
CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Pane
“Since no quantified virus isolates of the 2019-nCoV were available for CDC use at the time the test was developed and this study conducted, assays designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA (N gene; GenBank accession: MN908947.2) of known titer (RNA copies/µL) spiked into a diluent consisting of a suspension of human A549 cells and viral transport medium (VTM) to mimic clinical specimen.”
https://www.fda.gov/media/134922/download
The CDC test was recalled early on due to a number of false-positives that were blamed on contamination and they ended updating the test to the N2 US CDC. However, this didn't work out too well as even the new test, along with the Drosten test, were shown to produce false-positives in an independent analysis. Both PCR's turned up “SARS-COV-2” positive results in every sample tested, including negative control samples as well as water:
Performance Assessment of SARS-CoV-2 PCR Assays Developed by WHO Referral Laboratories
“The E Charité and N2 US CDC assays were positive for all specimens, including negative samples and negative controls (water). These false-positive results were explored (details below), but the sensitivity of these assays was not further assessed.”
“No false-positive results were obtained on clinical samples that tested negative for SARS-CoV-2 and/or positive for other viruses than SARS-CoV-2, except for E Charité and N2 US CDC, which were positive for all specimens.”
“It is worth noting that the Charité assay was the first to be published at the early stage of the pandemic [9] and has been widely used worldwide [8].”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7355678/
It should be clear to see how PCR can be easily utilized to generate fraudulent cases in order to sell panic and fear over the exact same symptoms of disease that were never shown to be caused by any “virus.” This is why it was always a testing pandemic and never a “viral” one.
There was no new disease, no scientific evidence proving the existence of a “novel virus,” and no tests that could accurately detect the nonexistent “threat.” In every way possible, there was no reason to believe the mainstream media hype. However, the pharmaceutically financed MSM is a well-oiled machine that is capable of churning out convincing fear propaganda that is immediately consumed without question by the frightened public seeking protection. If people were to take the time to dig deeper beneath the terrifying headlines and attempt to read and understand the studies behind the words, they would have realized what more and more of the disenfranchised have come to understand throughout the last three years. There is no “Covid.” There are no “viruses.” Germ theory is an unproven and scientifically invalid theory. We have no reason to fear the invisible boogeymen as our health is in our own hands.
Please join us on June 20th, 2023 as we put the final nails in the coffin of this regularly scheduled programming. Germ theory and virology had their chance. The ratings are plummeting and the viewers are leaving in droves. The show is over. It is time to cancel it for good.


In order to flesh out some of the points made in the article, I wanted to provide a few relevant links:
For more on the lack of a specific disease known as “Covid,” please see this article:
Differential Diagnosis?

differential diagnosis : the distinguishing of a disease or condition from others presenting with similar signs and symptoms https://www.merriam-webster.com/dictionary/differential%20diagnosis I imagine most of us have “fond” memories of going to the doctor when feeling unwell and getting subsequently poked and prodded in order to determine a “cause” for t…
For more on the lack of “SARS-COV-2,” or any “coronavirus” for that matter, please see this article:
https://viroliegy.com/2021/12/24/creating-the-coronavirus/
For more on the problems with PCR, you can find plenty of information in these articles:
https://viroliegy.com/category/pcr-tests/
For more on the lack of an emergency, please see this article:
https://viroliegy.com/2022/03/07/wheres-the-emergency/
examined what it means for us now that the "pandemic” is officially over. explored whether or not mRNA even exists. provided an interesting look at the Marvin Haberland case in Germany that successfully challenged virology.

Sooner or later, fraudulent "science" will succumb to real science as people see more and more that our so called experts have huge conflicts of interest.
The new NIH director is basically "brought to you by Pfizer".
I don't think that's a smart choice these days, but hey, more open corruption just helps wake people up.
I have learned that most people are taught false notions most of their time in education, and that it is extremely difficult to question false beliefs that are protected by the idea of normalcy, peer pressure and scientific consensus.
Exploiting intellectual laziness is a very useful for of population control, far more useful than censorship, which is only the icing on the cake.
Thus, a pandemic is an economic, political and military issue, with only shallow connections to the natural sciences.