


The Healthy Sick
Fear the walking healthy. 🧟♂️


“In areas where there are limited number of new cases, State or local public health officials may request to test a small number of asymptomatic 'healthy people,' particularly from vulnerable populations”
-CDC Revised Guidelines August 2020
https://www.google.com/amp/s/www.cnbc.com/amp/2020/08/26/cdc-quietly-revises-coronavirus-guidance-to-downplay-importance-of-testing-for-asymptomatic-people.html
In the not so distant past, when we walked around feeling healthy without any symptoms of disease, most of us would consider that we were, in fact, free of any disease. There would be no thoughts about going to the doctor for a PCR test in order to determine whether or not we were unknowingly a walking talking “virus” spewing host harboring billions of “infectious” particles capable of transmitting disease to our loved ones. We would not subject ourselves to quarantines and daily testing due to the remote possibility of being around someone who tested positive with symptoms, let alone for anyone testing positive without any signs of disease. We did not go around covering our faces with masks out of fear that those around us may be silent spreaders. We didn't bust out our rulers in order to measure 6 feet of distance between us and another living soul. None of these irrational actions were ever even a glimmer of a thought until the well-orchestrated fear propaganda campaign promoted the pseudoscientific concept of the asymptomatic carrier of disease and catapulted it into the public consciousness.
Even though this idea has been effectively weaponized against us over the last few years, it is not a new one. In fact, as will be shown later, the notion of the asymptomatic carrier began at the same time germ theory was born. The idea is that one can be silently harboring and able to transmit a pathogen without displaying any symptoms of disease whatsoever. This has resulted in the highly illogical creation of asymptomatic disease:
What Does it Mean to Have an Asymptomatic Disease?
“Asymptomatic disease is where a person is infected with a disease (or develops a disease; diagnosed) but fails to display any noticeable symptoms.”
Asymptomatic until symptomatic – silent diseases
“Many diseases and infections can be asymptomatic, including those that may be potentially fatal in some people. These include (but are not limited to): tuberculosis, breast cancer, endometriosis, HIV/AIDS, herpes, hepatitis, chlamydia, hypertension, common colds/flu, and type-2 diabetes mellitus. Many of these conditions remain largely asymptomatic until very advanced disease stages when they suddenly become symptomatic. Others can remain more or less asymptomatic throughout their disease course.”
“Infectious diseases can also be completely asymptomatic (with no symptoms ever manifesting), particularly in younger and healthier individuals. For example, hepatitis (hepatitis C) infections can take up to 6 months to develop, and even then, approximately 80% of infected individuals may not experience any symptoms. Other examples include cholera, herpes, measles, and rubella which can be completely asymptomatic.”
“In summary, asymptomatic disease refers to diseases and infections which do not lead to any symptoms in patients (subclinical) for the whole disease course or until they develop symptoms in which the asymptomatic phase is referred to as pre-symptomatic.
In many respiratory infections including COVID-19, asymptomatic disease is common and may be a source of transmission within the community, though more research is needed to establish the exact contribution asymptomatic transmission has on the community rates of infection.”
As can be seen, many so-called “infectious diseases” are said to be asymptomatic. If one is labelled as asymptomatic, one never develops the disease at any point in time even though they are diagnosed with asymptomatic disease. This is a pseudoscientific concept that is also an oxymoron as two entirely contradictory terms were put together in order to create this illogical state. Asymptomatic is characterized by a lack of signs and symptoms of illness, whereas disease is characterized by signs and symptoms of illness. One can not have disease if one is not displaying signs of disease:
Asymptomatic carriers are nothing but healthy people who have been labelled with disease minus signs of any disease who are then told that they can infect others. They are treated as a sick individual based upon results generated using fraudulent tests. In the past, most would have scoffed at this idea and never willingly subjected themselves to quarantines and further testing. In fact, they would have never tested to begin with. However, in the face of a “pandemic” with a “novel virus,” many lined up for the mass testing agenda in order to ensure that they were amongst the “uninfected.” This willingness to subject to testing despite a clear lack of symptoms was primarily driven by fear. This old concept was thrust onto a frigthened population and then ramped up in a way that had never been done so before.
In order to understand why there was never any reason to ever participare in this irrational belief of such a ridiculous concept, let's examine how the asymptomatic carrier first came about at the dawn of germ theory. We will then examine how this idea was weaponized against the public during the “pandemic” despite a complete lack of any scientific evidence in support of the asymptomatic disease carrier.

When German bacteriologist Robert Koch was looking for the causative agents of certain diseases in the late 1800's, he formulated a series of four logical requirements that needed to be met in order for anyone to claim that a certain microbe caused a specific disease. These were as follows:
The microorganism must be found in abundance in all hosts suffering from the disease but should not be found in healthy hosts.
The microorganism must be isolated from a diseased host and grown in pure culture.
The cultured microorganism should cause the same symptoms of disease when introduced into a healthy host.
The microorganism must be re-isolated from the inoculated, diseased experimental host and shown to be identical to the original causative agent.
While these logic-based postulates were accepted by and large within the scientific community, Koch quickly discovered a problem with his very first criterion. Whether it was tuberculosis, typhoid, malaria, or cholera, the microbe that he was claiming as causative agents were regularly found in healthy individuals. Thus, Koch was unable to satisfy his very own first Postulate. However, rather than realize that his criteria had worked as he had envisioned and had actually ruled out bacteria and other microbes as a causative agent of disease, Koch allowed for himself and others to bend not only his first postulate, but the others as well. Allowing for the bacteria and other microbes claimed to be causative agents of disease to be found in those without disease lead to the creation of the illogical concept that became known as the asymptomatic carrier of disease. Koch's entire claim to fame rested entirely on the perception that he was a microbe-hunter. Bending his own rules saved Koch from giving up his prestige, kept his findings intact, and helped to establish the germ theory on unfalsifiable pseudoscientific grounds.

Koch's idea of asymptomatic “infection” received a big push shortly afterwards when the media released propaganda promoting the idea of an asymptomatic carrier in 1907 by targeting an Irish immigrant by the name of Mary Mollen. Mary was a cook for wealthy families and ended up employed by banker Charles Henry Warren when he rented a summer home for himself and his family. When 6 of the 11 family members came down with the symptoms of typhoid fever over the last week of August, the property owners feared that no one would rent the house again if they believed that the property was the source of the outbreak. A man named George Roper was hired to investigate the situation and he came to the conclusion that it was Mary who had passed on the bacteria to the family through her cooking. This led to a modern day witch-hunt for Mary who refused to believe that she was the source of illness. Sadly, Mary was eventually involuntarily quarantined for the majority of the rest of her life. This ordeal led to Mary being notoriously and unfairly known by the moniker Typhoid Mary, even though many of her stool samples came back negative for the bacterium:
Typhoid Mary: the Tragedy of Mary Mallon
“On 11 November 1938, a 69 year old Irishwoman died on North Brother Island, New York. She had been held in isolation for 23 years, yet she had not been charged or convicted with any criminal offence.
Mary Mallon was born in Cookstown, Ireland in 1869. She immigrated to America when she was a teenager and found employment in domestic service. She developed an aptitude for cooking, and as this paid more than basic service, Mary accepted several jobs as a cook for the wealthy. In 1906, Charles Henry Warren, a New York banker, rented a summer home for himself and his family on Long Island. Mary Mallon was engaged as a cook for the duration of their stay. From the end of August, one by one people began to fall ill with typhoid fever, in all, six of the eleven occupants of the house developed typhoid fever.
The owners of the property feared that they would be unable to secure further tenants if the public believed that the source of the outbreak was their property and so hired Dr George Soper to investigate the cause. Soper came to the conclusion that Mary Mallon was to blame for the spread of disease. Hindering his efforts, Mary had left their employment three weeks after the outbreak. Soper started to investigate the previous situations held by Mary Mallon. From 1900 to 1907 there had been seven jobs where, it was reported, somewhere between twenty-three and thirty-eight people became ill and one person, a child, died. Soper believed that Mary was the source of typhoid fever that had followed her employment history, but he needed biological samples to affirm his hypothesis.”
“The Greater New York Charter allowed for ‘all reasonable means for ascertaining the existence and cause of disease’. It essentially gave health officials the authority to remove Mary Mallon and quarantine her against her will. After two years of isolation, with only a dog for company, Mary sued the health department. They had tested her stools approximately weekly and 120 out of 163 samples proved positive. Yet Mary countered with her own private analysis, sampled over the preceding year, all coming back negative. Mary’s laboratory results proved for her, her healthy status and she failed to understand that she was diagnosed a healthy typhoid carrier. She was arguably the first person identified as such, and having not been charged with a criminal offence she felt it was barbaric to be treated like a criminal (and a ‘leper’) when she was innocent of any crime.”
https://historianruby.com/2017/11/02/typhoid-mary-the-tragedy-of-mary-mallon/
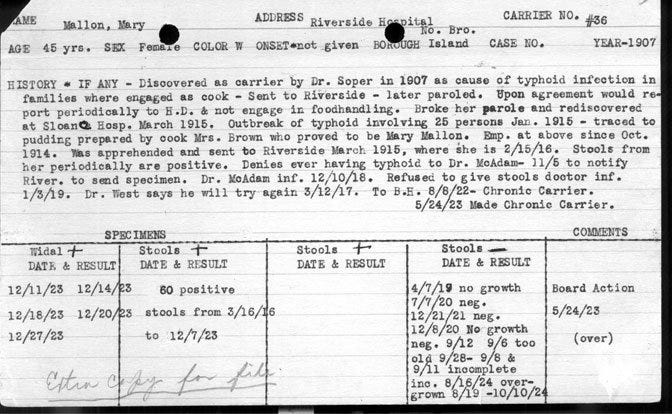
Mary was falsely quarantined against her will due to one man's suspicion and hypothesis that rested solely on correlation equaling causation. No scientific experiments were ever carried out proving that Mary was spreading disease to her patrons. As with all claims of asymptomatic transmission, it was a circumstantial case built upon faulty epidemiological data. George Roper is the man who ultimately condemned Mary by labeling her as the cause without any scientific evidence proving his hypothesis. Based upon his own words presented below, he assumed certain premises, such as the bacterium should be in the urine (which it was not) and in the feces. He claimed that stool examinations only failed twice over the course of two weeks to find the bacterium. However, he later recounted several instances of failure to detect the bacterium over the course of several months. In the summer months, few bacterial colonies were found and in the month of July, there were five consecutive negative tests. During the month of August, no typhoid was ever found in Mary's stools. In September, they began to appear again. However, from September 11 to October 14, 1907, the stools failed to yield any typhoid bacilli. From October 16, 1907, to February 5, 1908, weekly examinations of the stools showed anywhere from 25 to 50 percent “typhoid-like” colonies on the culture plates. There were two instances within that period where no bacilli were found. Taking into account that Mary's own independent lab results showed that no bacilli were found within her stools, Soper's consistently contradictory evidence should have been questioned.
After recounting these failures, Soper shared his thoughts on how Mary transmitted the bacterium through having not washed her hands properly while preparing the food. He based his conclusion upon his interviews where he stated that no housekeeper ever told him that Mary was a clean cook. He did not say whether he asked them or not or rather just assumed that their lack of addressing it was proof that Mary was unsanitary. Soper then stated that, in the most thorough “investigation,” he believed that the bacterium was carried from Mary's hands to the people who ate ice cream containing cut-up peaches that she had prepared. Again, no evidence was provided beyond his belief. Soper was amazed that no one had ever discovered an asymptomatic carrier in America before him. Interestingly, Soper revealed that he was long interested in the transmission of typhoid fever and knew of Robert Koch's work. He stated that his interest in this area was longstanding and that Koch's work was the basis for his own investigation. He admitted that he had read several papers on the probable role of healthy carriers in producing typhoid. Soper was made aware by Dr. Simon Flexner, of the infamous Flexner report, to some of these references after he had concluded his work on the Mary Mallon case. It is very clear that Soper went looking for evidence to fit his preconceived conclusions as to what the cause was. He was also potentially guided along the way:
THE MILITARY SURGEON VOL. XLV JULY, 1919 NUMBER 1 ORIGINAL ARTICLES TYPHOID MARY
By Major GEORGE A. SOPER
“It was expected by me that the germs might be found in the urine, but more probably in the stools. None was found in the urine. The stools contained the germs in great numbers. Daily examinations made for over two weeks failed only twice to reveal the presence of the Bacillus typhoid and on these occasions the sample taken was perhaps too small to reveal them. The blood gave a positive Widal reaction. The cook appeared to be in perfect health.
The feces were examined on an average of three times a week from March 20 to November 16, 1907, and in only a comparatively few instances did the investigators fail to find the bacilli. During the summer months the culture plates contained only a few typhoid-like colonies. In July there were five consecutive negative tests followed by a positive one.
During August the stool showed no typhoid; in September they began to appear again; from September 11 to October 14, 1907, the feces failed to yield typhoid bacilli. During this time the patient’s diet was carefully regulated and she was receiving mild laxatives. On October 16, 1907, a very thorough test showed that the germs were again present. From October 16, 1907, to February 5, 1908, weekly examinations of the stools gave, with only two exceptions, from 25 to 50 per cent typhoid-like colonies on the culture plates. These exceptions were on November 13 and December 4, when no typhoid was found. The implication was plain. The cook was virtually a living culture tube in which the germs of typhoid multiplied and from which they escaped in the movements from her bowels. When at toilet her hands became soiled, perhaps unconsciously and invisibly so. When she pre-pared a meal, the germs were washed and rubbed from her fingers into the food. No housekeeper ever gave me to understand that Mary was a particularly clean cook. In the Oyster Bay outbreak, which was studied with more particularity than the others, the infectious matter is believed to have been carried from the cook’s hands to the people who were later taken sick by means of ice cream containing cut-up peaches. Mary prepared this herself. In this instance no heat sterilized the washings from her hands. Mary Mallon was kept virtually a prisoner by the Department of Health for three years. At first she was held at the hospital for contagious diseases at the foot of East 16th Street, Manhattan; later she was removed to Riverside Hospital on North Brother’s Island in the East River, between Hell Gate and Long Island Sound.”
“The case is least remarkable for the reason that it was the first of its kind to be worked out in America. It is surprising that nobody bad discovered a carrier before. They are now known to be rather common.
Somewhat similar investigations bad been made in Germany) and I make no claim of originality or for any other credit in her discovery. My interest and experience in the epidemiology of typhoid had been of long standing. I had read the address which Koch had delivered before the Kaiser Wilhelm’s Akademie, November 28, 1902, and his investigation into the prevalence of typhoid at Trier 3 and thought it was one of the most illuminating of documents. In fact it had been the basis of much of tile epidemic work with which I had been connected.
Koch’s address was not the only one printed about this time to show that healthy carriers might exist and give rise to typhoid. Conradi and Drigalski4 had anticipated Koch and it was probably on the suggestion contained in their paper to the effect that with their new culture medium they had found typhoid bacilli in the stools of several well persons that Koch’s flying laboratory was sent to Trier and the ground prepared for his Kaiser Wilhelm’s Akademic address.
In the Festschrift Zum SeclizigstenGeburstag von Robert Koch, which appeared in 1903, there are several papers on the probable role of healthy carriers in producing typhoid. About this time Kayser, Klinger and others were publishing in Arbeiten aus dem Kaiserlichen Gesundheit-smate reports of cases which they found to be due to persons whose condition was much like Typhoid Mary’s. Dr. Simon Flexner kindly called my attention to some of these references after I had concluded my work on the Mary Mallon case.”
https://sites.lsa.umich.edu/rbender/syllabus/george-soper-on-mary-mallon/
After the highly publicized Typhoid Mary case, this idea of asymptomatic carriers simmered in the background over the next century. While there were claims of such a state in certain diseases, this has never been scientifically proven. However, that did not stop Koch’s escape clause from taking a prominent role in the “Covid crisis,” primarily due to a mass testing campaign that was bound to identify positive cases in healthy people using fraudulent tests never calibrated and validated to purified and isolated “virus.” Although all PCR results are false-positives, we can see that even the CDC noted that testing people without symptoms generates false-positive cases. They stated as much under their PCR guidelines for pertussis when recommending not to test those without symptoms:
Diagnosis PCR Best Practices
“However, only patients with signs and symptoms consistent with pertussis should be tested by PCR to confirm the diagnosis. Testing asymptomatic persons should be avoided as it increases the likelihood of obtaining falsely-positive results. Asymptomatic close contacts of confirmed cases should not be tested and testing of contacts should not be used for post-exposure prophylaxis decisions.”
https://www.cdc.gov/pertussis/clinical/diagnostic-testing/diagnosis-pcr-bestpractices.html
Thus, we can see that the CDC were well aware that testing people without symptoms will lead to an influx of cases labelled as asymptomatic “infections” when they are, in fact, not “infected” or diseased at all. This massive amount of asymptomatic cases of “SARS-COV-2” based upon fraudulent test results has cemented the illogical concept of the asymptomatic carrier into the minds of the populace. A timely December 2020 review, while reiterating the history of the asymptomatic carrier described above, pointed out the fact that even though asymptomatic infection and transmission has always been a concept waiting it the wings, it has only recently been thrust into the limelight with this “pandemic:”
Invisible epidemics: ethics and asymptomatic infection
History
“Dr Robert Koch was one of the founders of modern microbiology, and his work is particularly well known for a set of postulates (first published in 1890) linking microbes with the causation of infectious disease (Gradmann 2010). Though variously expressed, one of Koch’s initial postulates was that the microbe putatively responsible for a disease should be found in all people suffering from the disease, but not in healthy individuals (Gradmann 2010). Koch soon realised that this did not hold true in all cases, since many potentially pathogenic organisms are frequently found in healthy people. For example, Koch observed that asymptomatic carriers of cholera, typhoid, and malaria could spread these diseases to others, and he is credited for inventing the concept of the carrier state (i.e., in which healthy people asymptomatically carry an infection) (Gradmann 2010).
Public awareness of asymptomatic carriage of infection increased, especially in English-speaking countries, with media reporting of the case of Mary Mallon (known as “Typhoid Mary”) beginning in 1907. Mallon was a cook working in New York who, although showing no signs of typhoid disease herself, spread typhoid bacteria to many other people, resulting in several deaths (Brooks 1996; Soper 1939). For the general population, this revealed an important truth: that “persons, rather than things” (Soper 1939) were the source of many infectious diseases. Despite this Copernican revolution in public health (an epidemiological parallel of the microbiological revolution of germ theory), Mary Mallon and many others found it difficult to believe that healthy people could spread disease. Mallon repeatedly resisted public health restrictions and refused to believe she was infected or posed risks to others. She spent the latter years of her life living in public health confinement on North Brother Island, working as an assistant in the local infectious disease laboratory (Soper 1939).”
Implications for outbreaks, epidemics, and pandemics
“Asymptomatic infection was recognised to be a significant factor in the 2015–2016 Zika virus epidemic, particularly because many of those who were infected—including some women who acquired infection during pregnancy and gave birth to children severely affected by congenital Zika syndrome—showed few or no symptoms (Jamrozik and Selgelid 2018). Although less well recognised, transmission of asymptomatic Middle Eastern Respiratory Syndrome (MERS) coronavirus infection (perhaps both camel-human and human–human transmission) may play an important role in the epidemiology of MERS—which is all the more remarkable because people who develop symptomatic MERS infection have a high fatality risk of around 35% (Grant et al. 2019). Asymptomatic infection has also been reported for viruses closely related to the coronavirus that caused the earlier severe acute respiratory syndrome (SARS) epidemic. In one study from 2003, around 40% of Chinese wild animal traders had serological evidence of having been exposed to coronaviruses that closely resembled SARS-coronavirus, raising questions about whether people in high risk occupations should be screened for asymptomatic infection to detect potential “spillover” events of pathogens with epidemic potential (Guan et al. 2003). We initiated the November 2018 Brocher Foundation workshop upon which this Special Issue is based partly in light of the growing awareness of such cases of asymptomatic infection—and their ethical implications for policy and practice.
Since that time general awareness of asymptomatic infection has skyrocketed in light of its role in the coronavirus disease 2019 (Covid19) pandemic, in virtue of which the term ‘asymptomatic infection’ has become highly familiar to ordinary members of the general public. Early data, which were later widely confirmed, suggested that asymptomatic transmission of Covid19 occurs both in cases where the individual transmitting the virus goes on to develop symptoms later (i.e., they were “pre-symptomatic” at the time of transmission) and in cases where they never develop symptoms (Hu et al. 2020). Asymptomatic individuals can, under certain conditions, transmit to large numbers of other people (e.g., one person was shown to infect 71 others) (Liu et al. 2020). The overall degree to which asymptomatic transmission contributes to local Covid19 epidemics likely varies in different contexts and has not always been well-characterised (in part because of the difficulties of identifying all asymptomatic infections during an epidemic). In any case, asymptomatic transmission of Covid19 raises a number of ethical issues similar to those discussed above, including those related to the justification of public health interventions such as screening and isolation for asymptomatic cases.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7738616/
While the asymptomatic carrier was made a star of the “Covid” show in order to generate fear and drive compliance towards quarantines, lockdowns, social-distancing, and masking, the message has been entirely inconsistent throughout, and the lack of any valid scientific evidence proving such a carrier state was on full display from the very beginning. At a White House press briefing on January 28th 2020, the idea of asymptomatically transmitting the “novel coronavirus” was floated out there as a possibility. The CDC claimed to have heard reports about asymptomatic cases but had not seen any of the data. At the time, poster boy Anthony Fauci stated that, based upon past evidence from respiratory “viruses” of any type, asymptomatic transmission was never a driver behind any outbreaks or spread of disease:
Asymptomatic transmission
“There’s a difference between someone who has the virus and is about to show symptoms and someone who gets it and never has any noticeable sign. The second type is purely asymptomatic and there was a lot of uncertainty on this point at a Jan. 28 White House briefing. The CDC said there were reports of it, but they hadn’t seen the data.
Fauci put the question into the context of past coronaviruses.
"We would really like to see the data because, if there is asymptomatic transmission, it impacts certain policies that you do regarding screening, etc. But the one thing historically people need to realize is that, even if there is some asymptomatic transmission, in all the history of respiratory-born viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person. Even if there's a rare asymptomatic person that might transmit, an epidemic is not driven by asymptomatic carriers."
https://www.politifact.com/article/2020/jul/14/context-trump-criticizes-look-back-faucis-early-co/
However, a few days later on February 3rd, 2020, Anthony Fauci had changed his tune and stated that, based upon a single paper, he had no doubt that asymptomatic transmission was occurring and that the study he had read had laid the case to rest. Unfortunately for Fauci, the conclusive evidence that asymptomatic transmission occurred was based upon false information. The study in question claimed that a woman, who had been in a meeting in Germany with four people who later became ill, was an asymptomatic carrier as she had no symptoms at the time of the meeting and became ill upon her flight home to China. For some reason, the authors of the paper failed to actually speak to the woman and wrote the paper solely based upon what the four patients told them. Ironically, the Robert Koch Institute actually spoke to the woman and confirmed that she was symptomatic at the time of the meeting, thus giving Fauci a nice serving of egg on his face:
“Chinese researchers had previously suggested asymptomatic people might transmit the virus but had not presented clear-cut evidence. "There's no doubt after reading [the NEJM] paper that asymptomatic transmission is occurring," Anthony Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases, told journalists. "This study lays the question to rest."
But now, it turns out that information was wrong.
The letter in NEJM described a cluster of infections that began after a businesswoman from Shanghai visited a company near Munich on 20 and 21 January, where she had a meeting with the first of four people who later fell ill. Crucially, she wasn't sick at the time: "During her stay, she had been well with no sign or symptoms of infection but had become ill on her flight back to China," the authors wrote. "The fact that asymptomatic persons are potential sources of 2019-nCoV infection may warrant a reassessment of transmission dynamics of the current outbreak.
But the researchers didn't actually speak to the woman before they published the paper. The last author, Michael Hoelscher of the Ludwig Maximilian University of Munich Medical Center, says the paper relied on information from the four other patients: "They told us that the patient from China did not appear to have any symptoms." Afterward, however, officials at the Robert Koch Institute (RKI), Germany's federal public health agency, and the Health and Food Safety Authority of the state of Bavaria did talk to the Shanghai patient on the phone, and it turned out she did have symptoms while in Germany. According to people familiar with the call, she felt tired, suffered from muscle pain, and took paracetamol, a fever-lowering medication. (An RKI spokesperson would only confirm to Science that the woman had symptoms.)”
https://www.science.org/content/article/paper-non-symptomatic-patient-transmitting-coronavirus-wrong

In March 2020, a top Chinese health official completely contradicted Fauci by stating that there was no evidence that asymptomatic carriers could spread illness to others:
‘No evidence’ asymptomatic carriers spread coronavirus, Chinese health official claims
“A top Chinese health official sought to allay growing fears over asymptomatic coronavirus carriers on Monday, saying there was “no evidence” they could spread the illness but medical workers should remain alert to the risk.”
Not one to be made the fool, in April 2020, Fauci suggested that there were millions of silent spreaders in the US. In fact, he claimed that asymptomatic infections made up anywhere from 25 to 50% of the infections. He backed his figures up by confidently stating that they were just guessing as they had no scientific data to support these guesstimates. Fauci stated that he wouldn't have any “scientific” data until mass antibody testing was carried out. He said that it was impossible to know who is infected without symptoms until you test everyone who has no symptoms. This lends credence to the fact that testing people without symptoms will, as the CDC stated with pertussis, create nothing but false-positives:
Fauci once dismissed concerns about 'silent carriers' of coronavirus. Not anymore.
At Sunday’s White House briefing, Dr. Anthony Fauci, the longtime director of the National Institute of Allergy and Infectious Diseases, suggested that hundreds of thousands — or even millions — of “silent carriers” may be unwittingly spreading the coronavirus across the United States because they don’t realize they’re infected.
The idea that at least some coronavirus carriers don’t feel sick isn’t new. But the scale of Fauci’s estimate was.”
“It’s somewhere between 25 and 50 percent” of the total, Fauci said. But “right now,” he went on, “we’re just guessing.”
“The first thing to note is that Fauci himself expressed a high degree of uncertainty about his own numbers. “I don’t have any scientific data to say that,” he admitted Sunday. “You know when we’ll get the scientific data? When we get those antibody tests out there and we really know what the penetrance is. Then we can answer the questions in a scientifically sound way.”
“Fauci was right to be cautious. As he noted, it’s impossible to say how many carriers never showed symptoms until you’ve tested a bunch of people who never showed symptoms — something that will only happen after the worst of the pandemic is over and scientists start trying to determine, en masse, who does and doesn’t have immunity. (More on that later.)”
“Last week Centers for Disease Control and Prevention Director Robert Redfield told NPR that “one of the [pieces of] information that we have pretty much confirmed now is that a significant number of individuals that are infected actually remain a asymptomatic."
In June 2020, the WHO's Maria Van Kerkhove disagreed with Fauci's assessment of asymptomatic transmission by claiming that it appears to be rare based upon the data that was seen. In fact, she claimed that investigators were not finding any cases of secondary transmission from an asymptomatic carrier to anyone else:
Coronavirus spread by asymptomatic people 'appears to be rare,' WHO official says
"From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual," Van Kerkhove said on Monday.
"We have a number of reports from countries who are doing very detailed contact tracing. They're following asymptomatic cases, they're following contacts and they're not finding secondary transmission onward. It is very rare -- and much of that is not published in the literature," she said. "We are constantly looking at this data and we're trying to get more information from countries to truly answer this question. It still appears to be rare that an asymptomatic individual actually transmits onward."
However, by November 2020, Fauci was defiant against the WHO's admittance that no secondary transmissions were occurring and stated that he was certain that 40-45% of the transmission was due to asymptomatic carriers. Fauci hammered home the point as to why masks, which he had claimed offered no protection in March 2020, were now essential in November 2020:
Anthony Fauci’s Thoughts on Covid-19 Transmission, Treatments, and Vaccines
“Speaking of asymptomatic spread, Fauci says that 40–45% of transmission is due to asymptomatic people unwittingly infecting others. This is why masks are so essential — by wearing one, you protect other people even if you don’t know that you’re infected.”
In December 2021, Fauci was defeated yet again when the “discoverer” of Omicron, Dr. Angelique Coetzee, questioned whether such a thing as an asymptomatic carrier even existed at all. She stated that they had seen no asymptomatic cases of Omicron and then recommended that those without symptoms need not test:
‘There’s no reason to test if you have no symptoms,’ and 2 other findings from the woman instrumental in first identifying omicron
“Notably, Coetzee suggested that asymptomatic cases of the omicron variant are rare, if such a condition exists at all.
Asked during a Christmas Eve interview on MSNBC if “there was not such a thing as an asymptomatic case of omicron,” Coetzee responded: “We haven’t seen it.”
Secondly, the chairwoman of the South African Medical Association also told MSNBC on Friday that she doesn’t recommend testing by individuals until, and if, symptoms arise from the variant. “There’s no reason to test if you don’t have symptoms,” she said.”

In another blow to the ego of “Science,” an April 2021 study published by the CDC saw Fauci's statements contradicted yet again when the researchers found no asymptomatic transmission. In fact, they stated that their findings were in line with other studies and that asymptomatic transmission was unlikely to contribute to the spread of “Covid,” which torpedoed Fauci's claims of 40-45% of transmission being due to those without symptoms:
Analysis of Asymptomatic and Presymptomatic Transmission in SARS-CoV-2 Outbreak, Germany, 2020
“We determined secondary attack rates (SAR) among close contacts of 59 asymptomatic and symptomatic coronavirus disease case-patients by presymptomatic and symptomatic exposure. We observed no transmission from asymptomatic case-patients and highest SAR through presymptomatic exposure. Rapid quarantine of close contacts with or without symptoms is needed to prevent presymptomatic transmission.”
Conclusions
“In this cluster of COVID-19 cases, little to no transmission occurred from asymptomatic case-patients. Presymptomatic transmission was more frequent than symptomatic transmission. The serial interval was short; very short intervals occurred.
The fact that we did not detect any laboratory-confirmed SARS-CoV-2 transmission from asymptomatic case-patients is in line with multiple studies (9–11).”
“In conclusion, our study suggests that asymptomatic cases are unlikely to contribute substantially to the spread of SARS-CoV-2. COVID-19 cases should be detected and managed early to quarantine close contacts immediately and prevent presymptomatic transmissions.”
https://wwwnc.cdc.gov/eid/article/27/4/20-4576_article
While Fauci's claims of asymptomatic transmission were obviously unfounded, there were many asymptomatic cases being generated due to the fraudulent testing, as predicted by the CDC with pertussis. Thus, the perception that asymptomatic people were spreading a “virus” was easily conveyed to the public based upon unscientific data. We can see evidence of the massive amounts of healthy people testing positive for a “virus” by way of the mandatory mass testing data that came out of China throughout the “pandemic.” For instance, in March of 2022, Shanghai reported that over 70% of their cases were asymptomatic.
Why is Shanghai seeing so many asymptomatic Covid-19 infections?
“China is in the grip of an Omicron wave, but about 70 percent of cases reported in March have not had any symptoms.”
“Of the 103,965 locally acquired cases reported in March, only 3,046 had symptoms, according to National Health Commission data. And most of the asymptomatic infections were reported in Shanghai.”
By November of 2022, China was seeing upwards of 90% of their reported cases described as asymptomatic.
China Reports Third Consecutive Daily Record for New COVID Cases
“China reported 35,183 new COVID-19 infections on Friday, of which 3,474 were symptomatic and 31,709 were asymptomatic, the National Health Commission said on Saturday, setting a new high for the third consecutive day.
That compared with 32,943 new cases a day earlier -- 3,103 symptomatic and 29,840 asymptomatic infections, which China counts separately.
Excluding imported cases, China reported 34,909 new local cases on Friday, of which 3,405 were symptomatic and 31,504 were asymptomatic, up from 32,695 a day earlier.”
By December 2022, China had given up on reporting their overwhelming amount of asymptomatic cases in their daily Covid counts:
China stops publishing asymptomatic COVID cases, reports no deaths
“China's National Health Commission (NHC) will as of Wednesday stop reporting new asymptomatic COVID-19 infections, as many people without symptoms no longer participate in testing, making it hard to accurately tally the total count, it said.”

There were many reasons provided for why China had so many asymptomatic cases but it easily boiled down to their untargeted mass surveillance testing of the entire population. It is clear that if one goes looking for cases, one will find them whether symptomatic or not. In China, it was very much the latter as they were seeing over 98% asymptomatic rates in Shanghai based upon their testing data. This goes against the idea that mass testing would find more symptomatic cases. As more healthy people were subjected to a fraudulent test, the more “healthy sick” people that could be added to the overall totals:
Explainer-Why are Shanghai's COVID infections nearly all asymptomatic?
“The number of new confirmed community transmitted cases in the major financial hub of Shanghai reached 4,477 on Tuesday, a record high, but only 2.1% showed symptoms. The share of symptomatic cases over the previous seven days was around 1.6%.”
“Following are some explanations for why the rate of asymptomatic cases is so high.
SURVEILLANCE TESTING
China is also the only major country to do mass, untargeted surveillance testing, which is bound to uncover more asymptomatic cases, although it could also be expected to reveal more symptomatic cases.
"Surely, high levels of testing will pick up more rather than less asymptomatic cases," said Adrian Esterman, an expert in biostatistics at the University of South Australia.”
https://www.yahoo.com/news/explainer-why-shanghais-covid-infections-094712100.html
Mass testing with fraudulent tests led to a surge in healthy people being fraudulently labelled as asymptomatic carriers. It doesn't matter that this very act of mass testing, as the CDC stated, increases the likelihood of false-positives (even though they are all false-positives). This perception of a massive number of “infections” of a “virus” regardless of any disease being present only helped to further solidify this illogical concept into the minds of a fearful public as if it were a scientifically proven fact when it is anything but. Ironically, despite their “test, test, test” mantra, the WHO actually claimed that its guidelines never recommended mass testing of asymptomatic people as was being done in China due to high costs involved and the lack of data of its effectiveness:
Analysis: Test, test, test? Scientists question costly mass COVID checks
“WHO guidelines have never recommended mass screening of asymptomatic individuals - as is currently happening in China - because of the costs involved and the lack of data on its effectiveness.”

Thus, we can see that there truly is nothing behind the claim of an asymptomatic carrier of disease other than the fraudulent label provided by technology never meant for diagnostic use, especially on such a massive scale as we witnessed during this “pandemic.” PCR can find anything in anyone and the result is utterly meaningless, as stated by inventor Kary Mullis:
“Anyone can test positive for practically anything with a PCR test, if you run it long enough with PCR if you do it well, you can find almost anything in anybody."
“[PCR is] just a process that’s used to make a whole lot of something out of something. That’s what it is. It doesn’t tell you that you’re sick, it doesn’t tell you that the thing you’ve ended up with really was going to hurt you or anything like that.”
The asymptomatic excuse was created in face of conflicting evidence by a man who wanted nothing more than to protect his prestige and his findings. Robert Koch was under pressure from a growing field of researchers who were either contradicting his own findings or making new discoveries of their own. Koch needed a way to ensure that his own research would stand up to scrutiny. Bending his own logical postulates in order to allow for the asymptomatic carrier to exist allowed for his contradictory findings, as well as those put forward by later researchers, to perservere in the face of any further challenges by opponents:
“Whatever I undertake these days, there will be a bunch of the envious and jealous at hand. They will try to challenge me and if they don’t succeed, try to make me turn away from my work in disgust.”
“Those happy days are gone when the number of bacteriologists was small and each of them could research wide areas in an undisturbed manner...So now in making the most modest and most careful delineation of a research area you will step on the first colleagues’ toes or bump into a second one unintentionally, or come too close to the third’s field of work. Before you even realise it, you are surrounded by opponents.”
-Robert Koch
https://pubmed.ncbi.nlm.nih.gov/20934644/
It is clear to anyone looking at the idea of an asymptomatic carrier of disease logically that this very notion does not stand up under scrutiny. This nonsense was summed up brilliantly by the late great Canadian researcher David Crowe:
"Someone who believes in the virus can explain this conundrum to me.
It has been strongly stated that asymptomatic people can be infectious for quite a long time (I can provide references if you don't believe me, but this has been widely stated). This means that for quite a long time their body has a large quantity of virus particles, otherwise infection wouldn't be possible. But their body doesn't react to these particles, an immune reaction would at least result in a fever. But without an immune reaction they can never get rid of the virus particles. And how is it that virus particles running around the body of some people don't do anything, whereas other people get seriously ill and die? How do all the virus particles in one person know that they shouldn't mess with the cells to cause symptoms, whereas in another person they all go crazy and cause devastation?
So we can conclude that (1) Asymptomatic people never get rid of the virus and therefore must be quarantined forever; (2) It's the virus that's deficient, not the person, which must mean there are multiple dramatically different strains; or (3) the viral theory is a load of BS.
Please help me."
-David Crowe March 31st, 2020
It is obviously number 3. The “viral” theory is a load of BS, and there is no such thing as a healthy sick person capable of transmitting disease. We have no reason to fear the walking healthy.




Omicron/Moronic. I wish more people would point that out. Not that it will matter. I've pointed it out to friends and family and received only blank stares. It went right over their heads. Intelligent people but their level of conscious awareness is in the toilet.
The story of Mary Mollen is a nightmare.