
Game of Clones
"When you play the game of clones, you win or you die. There is no middle ground."


“…human metabolism constantly generates a huge amount of RNA genetic sequences of many types and compositions that do not show up in form of DNA sequences in the chromosomes. This fact alone questions any claims concerning the existence of all RNA viruses, such as the corona viruses, Ebola viruses, HIV, the measles virus and the SARS viruses.”
-Dr. Stefan Lanka
https://truthseeker.se/the-virus-misconception-part-2-the-beginning-and-end-of-the-corona-crisis-by-dr-stefan-lanka/
It's a new year and with that comes certain expectations. For some, the new year brings a fresh start and a chance to build new relationships. For others, it is a time to finally accomplish goals that have remained unfinished for far too long. The start of each year is a time to reflect on attaining accomplishments and achievements that may have seemed unattainable in the past. It is a time to celebrate endings and proceed towards new beginnings. It is the motivational push many need to dream bigger and better.
Amazingly, it seems that this strive to be a better version of oneself does not stop with humanity. “SARS-COV-2 ” also got the memo that it is time once again to tackle the New Year’s resolution. The task for the little “virus-that-keeps-on-evolving” is to achieve its goal of becoming yet another more infectious version of itself so that it can continue to evade that pesky nuisance referred to as vaccine-induced “immunity.” Otherwise, if the “virus” stays the same and people continue to become ill, we might get the impression that these toxic injections are not effective whatsoever. Thus, it's a new year and the mainstream media is in full prep mode, hyping up the arrival of a brand new more-infectious “variant” ready to unleash havoc on the boosted, vaccinated, and unvaccinated alike:
“New Year, New Variant” seems to be the catchy slogan to start the year off right. For those who are uninformed, this discovery of yet another “variant” may seem like an ominous warning. CNN definitely wants us to be terrified of this prospect and sounded the alarm over the looming “variant” threat on New Year's Eve:
2022 ends with looming risk of a new coronavirus variant, health experts warn
“As the world enters a new year, many public health and infectious disease experts predict that monitoring for new coronavirus variants will be an increasingly important part of Covid-19 mitigation efforts -- and some are turning their attention to a surge in cases in China.
Subvariants of the Omicron coronavirus variant continue to circulate globally, and "we're seeing Omicron do what viruses do, which is it picks up mutations along the way that helps it evade a little bit of immunity that's induced by previous infection or vaccination," said Andrew Pekosz, a microbiologist and immunologist at the Johns Hopkins Bloomberg School of Public Health in Baltimore.
"We haven't seen any major jumps in terms of Omicron evolution in some time," he said. But "it's getting to that stage where it's something that we have to continue to monitor."
In the United States, the Omicron subvariants XBB.1.5, BQ.1.1, BQ.1, BA.5 and XBB are causing almost all Covid-19 infections, according to data from the US Centers for Disease Control and Prevention.
For this week, the CDC estimates that XBB.1.5 now causes 40.5% of cases in the US, followed by BQ.1.1 at 26.9%; BQ.1 at 18.3%; BA.5 at 3.7%; and XBB at 3.6%.
"SARS-CoV-2, the virus that causes COVID-19, is constantly changing and accumulating mutations in its genetic code over time. New variants of SARS-CoV-2 are expected to continue to emerge," CDC researchers write in their data tracker. "Some variants will emerge and disappear, while others will emerge and continue to spread and may replace previous variants."
“SARS-COV-2” had a head start on all of us in the race to complete New Year resolutions. For an unintelligent non-living entity, it is constantly seeking self-improvement. Due to its hard work paying off, we can't even just fear the “variants” like Omicron anymore. We must now cower in terror over the “subvariants” of the “variants” like XBB as well as the “variant” of the “subvariant” in XBB1.5, nicknamed “the Kraken,” a fearsome legendary sea-monster with numerous spikey tentacles.

Even the “prestigious” journal Nature got into the mix of fanning the flames of fear by questioning whether the “new subvariant” XBB1.5 is a global threat:
Is subvariant XBB.1.5 a global threat?
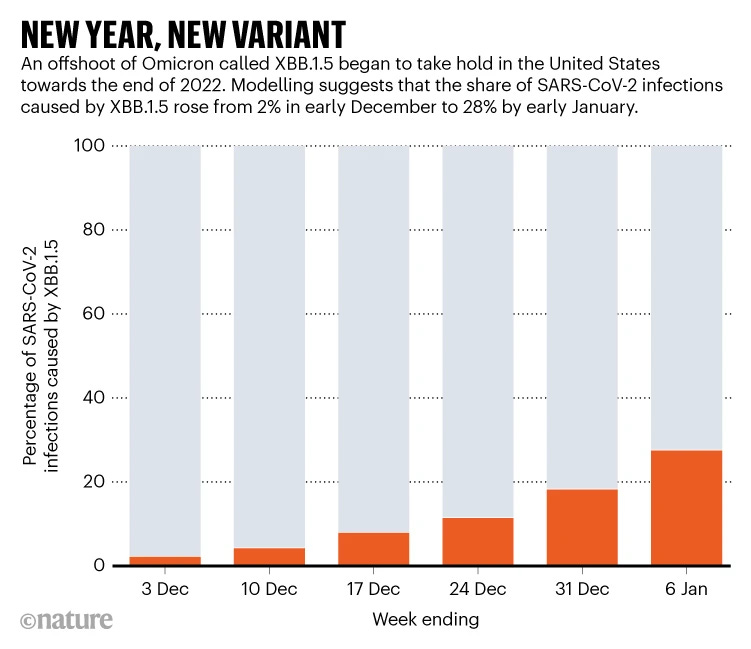
“A coronavirus subvariant called XBB.1.5 is on the rise globally — for example, scientists estimate that it is responsible for 70% of SARS-CoV-2 cases in the northeast United States. “It’s almost certainly going to dominate in the world,” says immunologist Yunlong Cao. The variant might not cause big waves of illness, thanks to pre-existing immunity, vaccination and boosters. But researchers will still be tracking the lineage closely. The subvariant bears a rarely seen mutation that might make it more infectious — and create an opportunity for evolutionary gains.”
https://www.nature.com/articles/d41586-023-00052-x
While this media push warning us over the threat of “the Kraken” may seem like a harbinger of doom that will surely lead to a surge in new cases, to those who are intimately familiar with this “variant” scam, this “New Year, New Variant” slogan means nothing more than the same old song and dance we have seen since the beginning. Sadly, many are still confused about how this scam works and unfortunately fall prey to media hype and propaganda. Thus, it seems like as good of a time as any to define what a “variant” is, examine some of the “variants” of the past three years, look at the interesting timing behind the emergence of each “variant,” and investigate the claims made about these potential threats. In doing so, it will be clear why there is absolutely no reason to fear “the Kraken” nor any other computer printout said to belong to a “virus.”
In order to get to the heart of this variant scam, the first thing that must be understood is that there is no scientific evidence proving the existence of any entity known as “SARS-COV-2.” No particles assumed to be the “virus” were ever purified and isolated directly from the fluids of a sick patient and proven pathogenic in a natural way. Instead, a genome for a hypothetical “virus” was assembled by way of computer algorithms from short fragments of RNA coming from the bronchoalveolar-lavage fluid (BALF) of one patient. This was an unpurified mixture containing many host, bacterial, fungal, and other unknown sources of RNA. The genome spit out from this mess served as the sole basis for German virologist Christian Drosten to create his own PCR test. He was able to conjure up a PCR test in a matter of days without having any purified and isolated “virus” on hand and based everything off of reports he saw on social media. Thus, “SARS-COV-2” only exists as fraudulently generated computer code stored in a database with cases spawned by a PCR test designed to detect small fragments of this invalid code.
As there is no purified and isolated “SARS-COV-2” found anywhere in the world, as brilliantly demonstrated by the FOI's gathered by Christine Massey, there can be no “variants” of an entity that was never scientifically proven to exist in the first place. So why are we being told about “variants” of a “virus” that does not exist in reality? The sequencing of “SARS-COV-2” is fraught with errors and biases. Each time the “virus” is sequenced in the computer, there are changes to the genome generated. These changes are claimed to be due to mutations rather than what they really are which is sequencing errors. These mutations are not found in the original “SARS-COV-2” genome and thus, any genome that differs from the original reference genome is classified as a “variant” as explained by virologist Vincent Racaniello:
“A virus variant is an isolate whose genome sequence differs from that of a reference virus. No inference is made about whether the change in genome sequence causes any change in the phenotype of the virus. The meaning of variant has become clouded in the era of whole viral genome sequencing, because nearly every isolate may have a slightly different genome sequence. Such is the case for SARS-CoV-2: nearly every sequence from a different person is slightly different. Up until the end of 2020, any SARS-CoV-2 sequences from any two individuals differed by about ten nucleotide changes out of 30,000. They are all variants, but the term is rarely used in this context. However since then viral genomes with many more changes have been identified. These have been called ‘variants of concern’ (VOC) because it is thought that the changes confer new phenotypic properties such as increased fitness. British scientists did a good deed by calling them VOCs, because now the press must call them variants.”
https://www.virology.ws/2021/02/25/understanding-virus-isolates-variants-strains-and-more/
According to Vincent Racaniello, nearly all, if not all, “SARS-COV-2” genomes are “variants” created any time the genome is sequenced. This view has been verified by other sources as well. According to chemist David Rasnick, no two “viral” genomes are identical, i.e. they are all variants:
“Viruses are unstable, RNA [e.g, SARS-Cov-2] viruses especially. They are so unstable, there is no such thing as an un-mutated RNA virus. They are like snow flakes, no two are identical.”
“None of the sequences of the world destroying [sarcasm], computer generated coronavirus with its 30,000 or so nucleotides, are identical.”
“The virus maniacs use computers to compare the menagerie of sequences to come up with ‘A Consensus Sequence’ for HIV, Coronavirus, and all the rest. The consensus sequence exists in two places: in computers and in strings of RNA synthesized in the lab.”
“Even consensus sequences are not stable. Different groups, using a variety of computer algorithms will invariably come up with different ‘consensus sequences’.”
-David Rasnick PhD chemist https://blog.nomorefakenews.com/2021/01/25/new-strain-of-coronavirus-or-a-giant-con/
An article in Nature stated that any two “SARS-COV-2” genomes collected from anywhere in the world will differ on average by 10 RNA letters:
According to the University of Michigan Health Lab, mutations are present in each person's “SARS-COV-2” genome:
In other words, the geneticists have a really hard time putting the same 30,000 puzzle pieces back together in the correct order every time. They find random pieces that do not belong or are out of place in every genome sequenced. On average, there are around 10 mutations per genome. Why is this important? Here is how the CDC defines mutations:
“A mutation refers to a single change in a virus’s genome (genetic code).”
From the same source, here is the CDC's definition of a “virus variant:”
“A variant is a viral genome (genetic code) that may contain one or more mutations.”
https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html
As it only takes a single mutation to be called a “variant” and every genome sequenced from each individual has on average 10 mutations, we can conclude based upon the information from these sources that all “SARS-COV-2” genomes are considered “variants.” Not a single one of these puzzles are able to reflect the original picture identically. According to GISAID.org, there are, at the time of this writing, over 14.5 million “SARS-COV-2” genomes in the database:
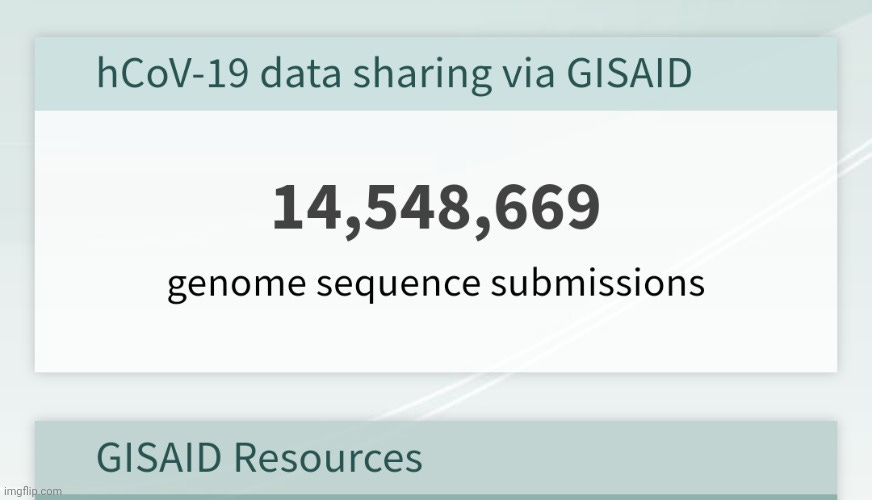
Thus, there are millions of “variants” at all times, every time a new sequence is submitted. This may lead one to wonder what is so special about XBB1.5 and the rest? Depending on where these incorrect pieces are found within the genomes of these “variants,” researchers will make interpretations as to whether they believe the A,C,T,G that are out of place in one computer printout makes it more transmissible and/or lethal than another printout. Once they determine that these mutations are significant based upon their assumptions about what these letters mean, they sound the alarm and the world is alerted of the arrival of a new “variant” of the original “virus” that never existed to begin with.
Some may think that this explanation of “variants” makes sense given the story that “viruses” mutate over time. However, this mutation excuse is used to cover up for the inability of these researchers to create the same puzzle every time. These mutations didn't just pop up after months of the “virus” circulating and “infecting” helpless victims. They were immediate as shown by the fact that the first 5 “SARS-COV-2” genomes were not identical:
A pneumonia outbreak associated with a new coronavirus of probable bat origin
“Full-length genome sequences were obtained from five patients at an early stage of the outbreak. The sequences are almost identical and share 79.6% sequence identity to SARS-CoV.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7095418/
They couldn't find the same exact “virus” within the first 5 patients but this apparently did not concern the researchers and they kept on chugging along, filling the database with more fraudulent genomic sequences. It took all of less than a month for the first concerning variant to arrive in late January with a D614G substitution, a mutation said to be a change to the spike protein which allowed for the “virus” to be more infectious. This “variant” was to become the dominant form of the “virus” by June 2020, right in time for the summer travel season. This conveniently set up the excuse for why, despite the lockdowns and quarantines, we saw a “surge” in cases. Of course, the increase in testing apparently had nothing to do with the sudden surge. It was the more “infectious variant:”
D614G

“A variant of SARS-CoV-2 with a D614G substitution in the gene encoding the spike protein emerged in late January or early February 2020. Over a period of several months, the D614G mutation replaced the initial SARS-CoV-2 strain identified in China and by June 2020 became the dominant form of the virus circulating globally. Studies in human respiratory cells and in animal models demonstrated that compared to the initial virus strain, the strain with the D614G substitution has increased infectivity and transmission. The SARS-CoV-2 virus with the D614G substitution does not cause more severe illness or alter the effectiveness of existing laboratory diagnostics, therapeutics, vaccines, or public health preventive measures.
https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON305
As the summer surge slowed down with the coming of the fall season and children returned to schools masked, sanitized, and social distanced, a new “variant” was said to be discovered in September 2020. Granted, this “variant” was retroactively placed to September 2020 as it did not start generating headlines until December 2020 when the mainstream media needed to provoke fear in order to increase demand for the vaccines which had rapidly descended upon us in November 2020. The B.1.1.7 “variant” was claimed to be discovered due to a number of PCR tests missing a signal in the all important S-gene for the spike protein. While this is normally considered a fault in the PCR tests which is known as the S-gene dropout, it was decided that, in these cases, it was not an error on the part of the test but was instead the work of a pesky new “variant.” Due to the testing failure to detect the spike protein, it was stated that not only was B.1.1.7 more infectious, it was also more deadly. Sounds like the perfect escape clause for an increase in illness and death due to experimental vaccine injuries:
Alpha (B.1.1.7)

“The B.1.1.7 variant, first spotted in the UK, is not only more easily transmitted, but it also appears to be more deadly. Dr. Anthony Fauci warned about it Friday in a White House coronavirus update.”
"Of concern is that there are about 50% increase in transmission with this particular variant that has been documented in the UK and there's likely an increase in severity of disease if infected with this variant," he said.
Fauci pointed to one study showing a 64% increased risk of death for people infected with B.1.1.7 compared to those infected with the older, so-called wild-type variant. He showed a second study that indicated a 61% higher risk of death with B.1.1.7.
But vaccines appear to protect well against B.1.1.7 and treatments such as monoclonal antibodies also appear to work against this particular variant, Fauci said.
That makes it more important than ever to get people vaccinated quickly, he said.
"The way we can counter B.1.1.7, which is a growing threat in our country, is to do two things: To get as many people vaccinated as quickly and as expeditiously as possible with the vaccine that we know works against this variant and, finally, to implement the public health measures that we talk about all the time ... masking, physical distancing, and avoiding congregant settings, particularly indoors," he said.”
https://www.google.com/amp/s/amp.cnn.com/cnn/2021/03/20/health/variant-b117-vaccines-work/index.html
After a few months of people willingly rolling up their sleeves for the experimental toxic injections, the world was alerted to the South African “variant” known as B.1.351. This update was discovered in Zimbabwe in February 2021. While it was claimed that this “variant” did not cause an increase in disease severity, it allegedly led to a higher “viral” load which meant that it was, once again, “more transmissible and infectious.” However, due to the out-of-place A,C,T,G's in the receptor-binding domain (RBD), it was decided that this “variant” could impact the effectiveness of the vaccines, leading to a convenient scapegoat for the ineffectiveness of the new vaccines:
Beta (B.1.351)
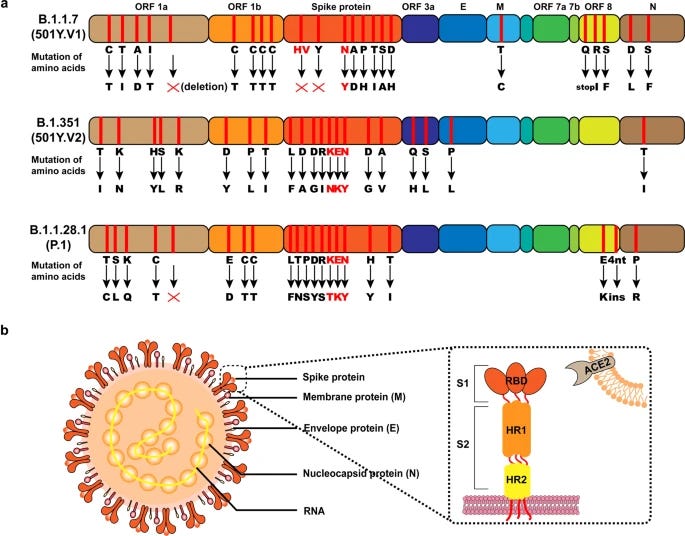
“B.1.351 is linked to higher viral load and increased transmission. While additional cases may stress already overloaded hospitals and systems, there is currently no evidence that B.1.351 is associated with increased severity of disease.”
“B.1.351 has multiple mutations in the spike protein, three of which are in a key region called the receptor binding domain (RBD).2 One mutation (N501Y) is the same as in the UK variant, which may be causing increased viral load and therefore increased transmissibility in both variants, but scientists do not believe the N501Y mutation will directly affect efficacy of the vaccines.
For B.1.351, which harbors additional mutations in the RBD (E484K and K417N), the effectiveness of vaccines is still a concern as recent research from Dr. Bloom’s lab at Fred Hutchinson Cancer Research Center has shown. While further research is rapidly being conducted to understand more about the bevy of mutations in these variants and their potential impact on vaccines, scientists around the globe remain hopeful.”
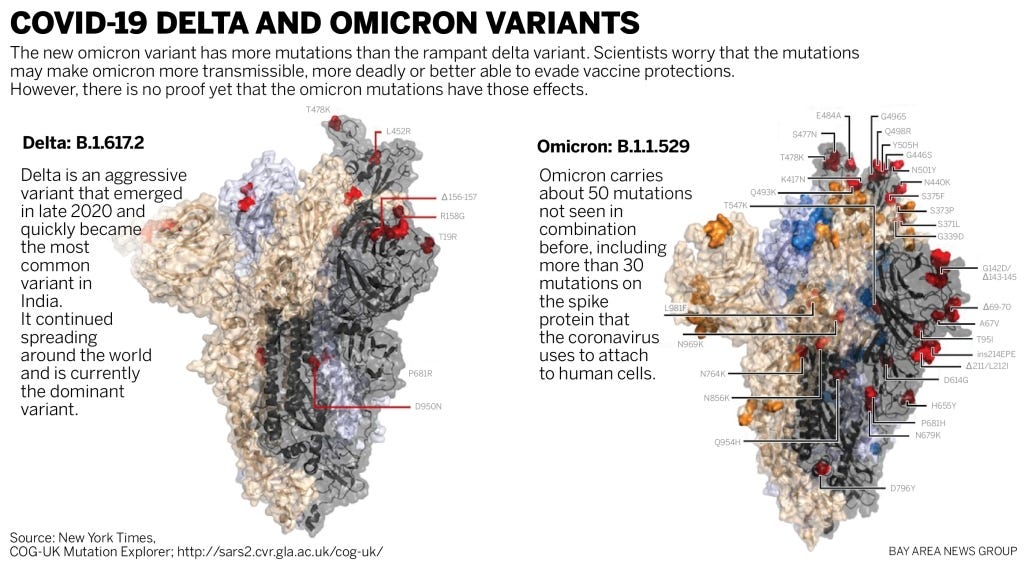
Right in time for increased “infections” due to the easing of restrictions (such as lockdowns and masking) and ready to be used as an excuse for the 2021 summer surge, the Delta “variant” made its presence known. While it was estimated to be circulating within the US in May 2021, it was claimed by the CDC to be the dominant “strain” heading into August 2021. This time, the vaccination campaign was in full swing yet “infections” were still occurring amongst the vaccinated in what were being called “breakthrough infections.” In order to explain away the obvious ineffectiveness and toxicity of the vaccines, the more contagious and deadly Delta arrived to save the day. It was stated that even those who were fully vaccinated could get the Delta “variant” and could still pass the “virus” on. This “variant” even produced the same “viral” load in both vaccinated and the unvaccinated. Suddenly, that sweet protection promised to those who took the toxic plunge didn't look so great after all. Thus, Delta struck at the perfect time in order to drum up increased fear in order to get more needles into the arms by way of the first fall booster campaign:
Delta (B.1.617.2)

“The Delta variant is more contagious: The Delta variant is highly contagious, nearly twice as contagious as previous variants.
Some data suggest the Delta variant might cause more severe illness than previous strains in unvaccinated persons. In two different studies from Canada and Scotland, patients infected with the Delta variant were more likely to be hospitalized than patients infected with Alpha or the original virus strains.
Unvaccinated people remain the greatest concern: Although breakthrough infections happen much less often than infections in unvaccinated people, individuals infected with the Delta variant, including fully vaccinated people with symptomatic breakthrough infections, can transmit it to others. CDC is continuing to assess data on whether fully vaccinated people with asymptomatic breakthrough infections can transmit. However, the greatest risk of transmission is among unvaccinated people who are much more likely to contract, and therefore transmit the virus.
Fully vaccinated people with Delta variant breakthrough infections can spread the virus to others. However, vaccinated people appear to be infectious for a shorter period: Previous variants typically produced less virus in the body of infected fully vaccinated people (breakthrough infections) than in unvaccinated people. In contrast, the Delta variant seems to produce the same high amount of virus in both unvaccinated and fully vaccinated people. However, like other variants, the amount of virus produced by Delta breakthrough infections in fully vaccinated people also goes down faster than infections in unvaccinated people. This means fully vaccinated people are likely infectious for less time than unvaccinated people.”
https://stacks.cdc.gov/view/cdc/108671
After getting those fall booster shots into the arms of the fearful, Omicron decided to pop up late November 2021 to explain away anyone who was now double-vaxxed and boosted who continued to test positive for the “virus” they were supposed to be protected against. While it was claimed to be not as deadly, Omicron was considered significantly more transmissible than Delta and overtook it as the dominant “variant” in just 4 weeks. The same PCR S-gene dropout failure that was determined as a way to identify Alpha was instead being used as a proxy for this new “variant” in order to generate cases. Omicron was said to impact the vaccines, as effectiveness against infection, disease, hospitalization and death began waning over time. Of course, this led to an increased urgency to get even more people double-vaxxed and boosted against the new threat:
Omicron (BA. 1)
“Omicron was quickly identified as being significantly more transmissible than Delta, the preceding variant of concern. Within 4 weeks, as the Omicron wave travelled around the world, it replaced Delta as the dominant variant.
Countries which had so far been successful in keeping COVID-19 at bay through public health and social measures now found themselves struggling. For individuals, the greatest price was paid by those who were at risk of severe disease but not vaccinated, and we saw hospitalizations and deaths rise in a number of places around the world.
By March 2022, WHO and partners estimate that almost 90% of the global population had antibodies against the COVID-19 virus, whether through vaccination or infection.
Overall, though, this new variant caused less severe disease than Delta on average. Scientists worked to understand why this was so. A number of factors likely played a role. For example, the virus replicated more efficiently in the upper airway, and population immunity had been steadily increasing worldwide due to vaccination and infections.
While vaccines reduced the impact of Omicron, they themselves were impacted: studies have shown that vaccine effectiveness against infection, disease, hospitalization and death waned (though at different rates) over time. However, protection against hospitalization and death have remained high, preventing millions of people from dying.”
https://www.who.int/news-room/feature-stories/detail/one-year-since-the-emergence-of-omicron
If one new “variant” was not enough to worry about at the start of 2022, you were in luck as Omicron kept the fear-train rolling with the introduction of the “subvariant” BA.2, otherwise known as Stealth Omicron. This “variant” of the “variant” of the computer printout “virus” was unable to be detected by way of the PCR S-gene dropout. Thus, it was claimed that this “variant” was difficult to distinguish from the previously dominant “strain” known as Delta. In other words, as Delta was phased out of the pipeline, Stealth Omicron was allowed to take its place. BA.2 was classified as a “variant of concern” (VOC) by the WHO as it was determined to be 1.5 times more transmissible than the already super transmissible Omicron. Instead of the vaccines and restrictions ending the “pandemic” as promised, this sneaky little bugger kept things right on track until the next “variant” could take its place. By April 2022, Stealth Omicron not so stealthily snuck its way to the top spot as the dominant “strain:”
Stealth Omicron (BA.2)
“The World Health Organization (WHO) is currently monitoring the original Omicron variant, BA.1, along with several additional subvariants BA.1.1, BA.2 and BA.3. The subvariant BA.2 has been referred to as “stealth” Omicron because it has genetic mutations that could make it harder to distinguish from the Delta variant using PCR tests as compared to the original version of Omicron.
The Omicron variant has been classified as a variant of concern by the WHO and the Centers for Disease Control and Prevention (CDC). The WHO has indicated that since BA.2 is Omicron, it is a variant of concern.
The Omicron variant spreads more easily than the original SARS-CoV-2 strain of the virus that causes COVID-19, and previous variants, including Delta. According to Danish scientists, the Omicron subvariant BA.2, is 1.5 times more transmissible than the original Omicron strain. While there is currently no evidence that the BA.2 lineage is more severe than the BA.1 lineage, experts have warned that BA.2 could extend the current wave of COVID-19 infections in the U.S.”
https://www.ama-assn.org/delivering-care/public-health/what-ba2-or-stealth-omicron-subvariant
Right before the Stealth Omicron became the leader of the pack, there was a little hullabaloo over a supposed recombinant version of “SARS-COV-2.” In March 2022, a Delta “variant” decided to merge with an Omicron “variant” after a magical first date together. This union resulted in the birth of an entity so ridiculous, it quickly faded into obscurity as a lab artifact: Deltacron! This freak of nature, however, was not viewed as a concern. Amazingly, this lack of concern was not due to its laughable moniker but because it was said to be “rare” and showed no signs of spreading exponentially. Eventually, the “experts” decided that this red-headed step-child was, in fact, an aberration either due to contamination, lab error, or technological artifact (aren't they all?). This fiasco led to GISAID.org urging caution when interpreting the A,C,T,G's and declaring the findings of new “variants:”
Deltacron (Variant or Contaminant?)

“The identification of Deltacron led to widespread news coverage and much debate on social media, but experts have questioned the findings, particularly those in Cyprus.
Dr. Jeffrey Barrett, Director of the COVID-19 Genomics Initiative at the Wellcome Sanger Institute in the United Kingdom, believes the findings are due to a lab error.
“This is almost certainly not a biological recombinant of the Delta and Omicron lineages,” he says. “The apparent Omicron mutations are located precisely and exclusively in a section of the sequence encoding the spike gene (amino acids 51 to 143) affected by a technological artifact in certain sequencing procedures.”
Writing on Twitter, Dr. Tom Peacock, a virologist at Imperial College London in the U.K, also dismissed the findings, saying that “[t]he Cypriot ‘Deltacron’ sequences reported by several large media outlets look to be quite clearly contamination.”
In a separate tweet, he nevertheless clarified that this was not due to poor lab practice, stating that it “happens to every sequencing lab occasionally.”
“In the meantime, researchers affiliated with the GISAID Initiative — a database that “promotes the rapid sharing of data from all influenza viruses and the coronavirus causing COVID-19” — have urged renewed caution when it comes to interpreting the data that allegedly indicate the emergence of a new sub-variant of SARS-CoV-2.
“[R]ushing to conclusions on data that have just been made available by labs that find themselves under significant time pressure to generate data in a timely manner is not helpful in any outbreak,” Cheryl Bennett, an official at the GISAID office in Washington, D.C., has told Nature.”
https://www.medicalnewstoday.com/articles/deltacron-new-variant-or-laboratory-error
While there were various other variants throughout the next few months (BA.3, BA.4, BA.5), there wasn't as much fanfare or media hype over these BA's. In July, there was a mini-fuss over the new Stealth Omicron nicknamed “Centaurus,” but alas, the Centaur didn't do much to sway the fear needle back to terror during the summer travel months.
The “variants” were losing their power to incite enough panic to drive the fearful to get vaccinated. Thus, it was left to the re-emergence of the “flu” and “RSV” and the threat of the Tripledemic to get the needles back into the arms. And as people are becoming sick once again from these toxic injections and they continue to test positive by way of the fraudulent PCR, we are now seeing the emergence of “the Kraken.” According to the WHO, this is the most contagious and transmissible version of the “virus” yet. Infections are doubling every week and while XBB1.5 may not be making people more sick, it is evading antibodies and vaccines like a champ. In other words, make sure not to blame the vaccines for XBB1.5's “Matrix-like” abilities to dodge the vaccine-induced antibody bullets. Just as the “scariants” did before, this unintelligent non-living entity evolved by changing its A,C,T,G's:
XBB (Omicron Subvariant)
“The XBB.1.5 omicron subvariant that's currently dominating the U.S. is the most contagious version of Covid-19 yet, but it doesn't appear to make people sicker, according to the World Health Organization.
Maria Van Kerkhove, the WHO's Covid-19 technical lead, said global health officials are worried about how quickly the subvariant is spreading in the northeastern U.S. The number of people infected with XBB.1.5 has been doubling in the U.S. about every two weeks, making it the most common variant circulating in the country.
"It is the most transmissible subvariant that has been detected yet," Van Kerkhove told reporters during a press conference in Geneva on Wednesday. "The reason for this are the mutations that are within this subvariant of omicron allowing this virus to adhere to the cell and replicate easily."
“Scientists say XBB.1.5 is about as good at dodging antibodies from vaccines and infection as its XBB and XBB.1 relatives, which were two of the most immune evasive subvariants yet. But XBB.1.5 has a mutation that makes it bind more tightly to cells, which gives it a growth advantage.”

Once you come to the realization that this pandemic was brought about by nothing but computer printouts with no physical entity backing these A,C,T,G's up, it becomes very easy to see the game for what it is. The original genome Frakensteined and assembled from the unpurified BALF of one patient was used to create PCR tests utilized to detect tiny fragments of a hypothetical model of a non-existent “virus.” As increasing cases are fraudulently detected and sequenced, more “variants” are added into the database to be interpreted by the researchers as to whether the sequence generated should be a cause for alarm. If the PCR test does not work properly and results in an S-gene dropout failure, a “variant” with a mutation to the spike protein can be assigned as the cause rather than admitting to a fault within the test itself to detect the all-important spike. Alarming tales can be spun about how these more contagious, more transmissable, more infectious, and more deadly “variants” are capable of evading every single measure used to “protect” us, whether it is lockdowns, quarantines, masking, sanitizing, vaccinating, etc. There will always be another “variant” that is able to do what the previous version could not as the common symptoms of detoxification seen every year will not go away. They need a “new” boogeyman at pivotal moments in order to explain away the failures and to keep the cattle terrified and heading towards the slaughterhouse. Thus, we get “New year, New Variant” as the next best scariant marches it way towards the castle in order to oust its less effective predecessor from the throne. However, we must keep in mind that there can be no “variant” of a hypothetical entity never scientifically proven to exist. Computer printouts from unpurified materials cobbled together into a hypothetical framework is being used to scare people into submission. This year, let's make a resolution to put a wrench in those plans and make sure that this game of clones comes to a fitting end.

Here are some related articles on “viral” genomes and “variants” from viroLIEgy.com:
The Case Against “Viral” Genomes
https://viroliegy.com/2022/03/09/the-case-against-viral-genomes/
Passage in Vero Cells: The Variant Game
https://viroliegy.com/2021/08/26/passage-in-vero-cells-the-variant-game/
The Variant Game: Fool Them Thrice…?
https://viroliegy.com/2021/11/30/the-variant-game-fool-them-thrice/
had an excellent open letter to Denis Rancourt regarding his investigation into the existence of "viruses."Dr. Tom Cowan always has amazing content and covered a lot of material in his latest Wednesday Webinar including a favorite topic of mine, the inability to differentially diagnose between “viruses.”
https://www.bitchute.com/video/Yi5yvgNmZwrM/
is a staple on this list for her and Dr. Mark Bailey's masterful content which includes their latest look at HPV and the toxic injections associated with it.
Mike are you aware that Li-Li Ren's team (a/k/a Little Dog team) used Hopkins clade exclusion software called KRAKEN II? This was used to cook up 402123.
9 likes? You should have 9 million, 90 million. 900 million. Anything but 33 million. Thanks Mike, great work as always.