


The Syphilis Scam: Ricord's Ruse
Setting the Stage.


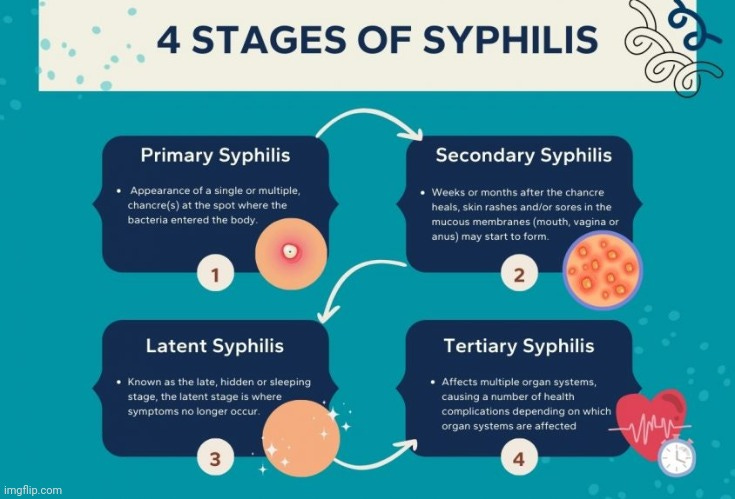
As syphilis is not really as common of a disease as it used to be prior to its replacement by HIV as the top STD in the 1980's, my guess is that most people are unfamiliar with how this illness supposedly works. I know that I, for one, was entirely unaware at the time that I found out about my relatives daignosis, that syphilis was a disease that supposedly attacked in stages. Normally, when most think of a disease, they think of an initial stage where the symptoms manifest which is ultimately followed by a gradual recovery. With syphilis, this is not the case as the disease is said to consist of 4 stages, each with their own signs and symptoms, or even an absence of symptoms. These stages are as follows:
Primary Syphilis
Secondary Syphilis
Latent Syphilis
Tertiary Syphilis
Primary syphilis is the first stage that is said to be accompanied by sores called chancres. According to the CDC, it can either be a single sore or multiple sores primarily found around the sexual organs. The Mayo Clinic states that “most people infected with syphilis develop only one chancre.” This sore can either be found pretty much anywhere on the body or never found at all. Both the CDC and the Mayo Clinic state that most people rarely notice if they even have a sore as they are typically painless and often hidden, which leads one to question whether these sores were ever present to begin with. The sore will even heal on its own without treatment:
Primary Stage
“During the first (primary) stage of syphilis, you may notice a single sore or multiple sores. The sore is the location where syphilis entered your body. These sores usually occur in, on, or around the
penis;
vagina;
anus;
rectum; and
lips or in the mouth.
Sores are usually (but not always) firm, round, and painless. Because the sore is painless, you may not notice it. The sore usually lasts 3 to 6 weeks and heals regardless of whether you receive treatment. Even after the sore goes away, you must still receive treatment. This will stop your infection from moving to the secondary stage.
Another interesting fact that many may be unaware of is that these sores, which the CDC admits will heal on their own, are often confused with many, if not all, other dermatological conditions, making clinical diagnosis next to impossible:
Syphilis: A Tricky Disease that may Pose Some Diagnostic Challenges - A Case Report
“However, from time to time the disease subtly comes to our clinic and, in many instances, poses difficulty for a clinical diagnosis. The difficulty in making a clinical suspicion of syphilis arises mostly from its great array of clinical manifestations, which, indeed, can mimic almost any dermatological diseases [4,5]. A common thought (and attitude) among clinicians is that when you do not know what it is, make syphilis as a possible diagnosis and screen the case serologically.”
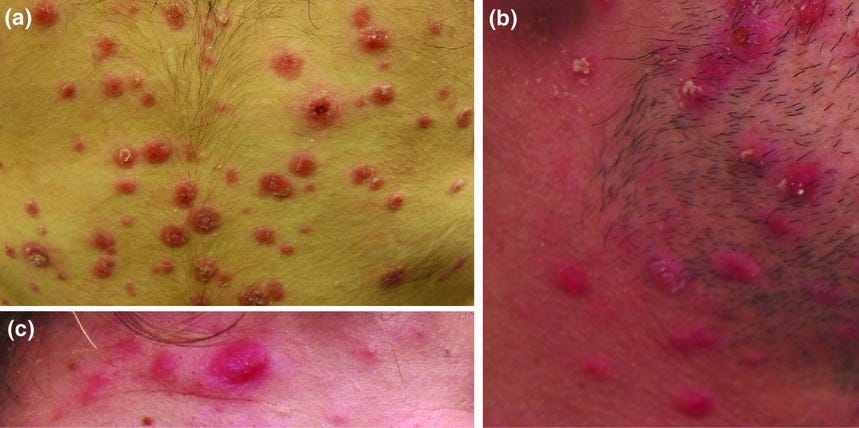
However, even though the sores associated with syphilis will admittedly heal on their own, the CDC urges people diagnosed with syphilis to seek treatment, otherwise they will encounter the second stage of the disease. This stage is known as secondary syphilis, and it is said to consist of rashes which can appear anywhere on the body. As with the chancres before them, the rashes may be so faint that people will not notice them. Along with possible unrecognized faint rashes, the usual flu-like symptoms, seen with every other disease, also accompany this stage. Just as with the symptoms from the first stage, the rash and flu-like symptoms will completely resolve on their own without treatment:
Secondary Stage
“During the secondary stage, you may have skin rashes and/or sores in your mouth, vagina, or anus. This stage usually starts with a rash on one or more areas of your body. The rash can show up when your primary sore is healing or several weeks after the sore has healed. The rash can be on the palms of your hands and/or the bottoms of your feet and look
rough;
red; or
reddish-brown.
The rash usually won’t itch, and it is sometimes so faint that you won’t notice it. Other symptoms may include:
fever;
swollen lymph glands;
sore throat;
patchy hair loss;
headaches;
weight loss;
muscle aches; and
fatigue (feeling very tired).
The symptoms from this stage will go away whether you receive treatment. Without the right treatment, your infection will move to the latent and possibly tertiary stages of syphilis.”
When we had to make the fateful decision for my relative to be treated for a syphilis diagnosis, we were told that this intervention would be to treat what is the next stage of the disease, known as the latent syphilis infection. According to their fictional narrative, those in this stage had survived through the initial two stages without treatment. However, now the sneaky bacteria had gone into sleep mode for some unknown reason and was hiding within the body. No symptoms of disease ever occur at this point in time and the person is said not to be contagious:
Latent Stage
“The latent (hidden) stage of syphilis is a period when there are no visible signs or symptoms of syphilis. Without treatment, syphilis will remain in the body even though there are no signs or symptoms. Early latent syphilis is latent syphilis where infection occurs within the past 12 months. Late latent syphilis is latent syphilis where infection occurs more than 12 months ago. Latent syphilis of unknown duration is when there is not enough evidence to confirm initial infection was within the previous 12 months. Latent syphilis can last for years.”
We were warned that without treatment, this latent infection could turn into what was known as tertiary syphilis. This is the final stage of the disease which is claimed to occur anywhere from 10-30 years after infection, although it is stated that this can occur at any time over the course of a person’s life. The bacterium supposedly reactivates for some reason after numerous years of slumber in order to destroy internal organs and eventually cause death. Obviously, this was terrifying to hear and ultimately led to the decision to accept the treatment. However, what we were not told, is that most people never experience this stage of the disease:
Tertiary Stage
“Most people with untreated syphilis do not develop tertiary syphilis. However, when it does happen, it can affect many different organ systems. These include the heart and blood vessels, and the brain and nervous system. Tertiary syphilis is very serious and would occur 10–30 years after your infection began. In tertiary syphilis, the disease damages your internal organs and can result in death. A healthcare provider can usually diagnose tertiary syphilis with the help of multiple tests.”
https://www.cdc.gov/std/syphilis/stdfact-syphilis.htm
We were also not told that the syphilis treatment did not have a standardized regimen or duration:
Treatment
“Because latent syphilis is not transmitted sexually, the objective of treating persons in this disease stage is to prevent medical complications of syphilis. Latent syphilis can also be vertically transmitted to a fetus; therefore, the goal of treating a pregnant woman is to prevent congenital syphilis. Although clinical experience supports the effectiveness of penicillin in achieving this goal, limited evidence is available for guiding choice of specific regimens or duration. Available data demonstrate that additional doses of benzathine penicillin G, amoxicillin, or other antibiotics in early latent syphilis do not enhance efficacy, regardless of HIV status (592,593,609).
https://www.cdc.gov/std/treatment-guidelines/latent-syphilis.htm
We were not told that most serological tests will turn up positive regardless of treatment and that most people remain positive for life. We were also not told that, as penicillin treatment was in use before randomized controlled trials became standard, the interpretations of the studies vary:
Syphilis: antibiotic treatment and resistance
“The latent stage of syphilis is the period from disappearance of secondary stage manifestations to the occurrence of the tertiary stage. Latent syphilis is divided into early latent (i.e. occurring within 1 year of infection) and late latent (i.e. occurring after 1 year of infection). While clinical symptoms are not apparent during latency, most serological tests are positive for antibodies to T. pallidum [Reference Seña, White and Sparling11]. About two-thirds of untreated syphilis patients remain in the latent stage for life.”
“Treponemal STS cannot be used to assess the response of patients to antibiotic treatment since patients with a positive test result usually continue to remain positive for the remainder of their lives, regardless of treatment.”
“Current regimens for treatment of syphilis were developed before randomized controlled trials became standard. Differences in interpreting earlier studies have resulted in some variability in national guidelines. However, penicillin, which was first used for treatment of syphilis in the 1940s, has remained the recommended first-line drug for treatment of all stages of syphilis.”
According to the WHO's standardized treatment recommendations for syphilis, we can see that these treatment recommendations are based on very low-quality evidence. These recommendations rely on the historical use of penicillin injections, which, as stated earlier, were studied prior to the standardization of randomized controlled trials. As usual, the recommendations are made because the WHO believes that the potential benefits outweigh the potential harms:
4.1. EARLY SYPHILIS (PRIMARY, SECONDARY AND EARLY LATENT SYPHILIS OF NOT MORE THAN TWO YEARS’ DURATION)
ADULTS AND ADOLESCENTS
RECOMMENDATION 1
In adults and adolescents with early syphilis, the WHO STI guideline recommends benzathine penicillin G 2.4 million units once intramuscularly over no treatment.
Strong recommendation, very low quality evidence
RECOMMENDATION 2
In adults and adolescents with early syphilis, the WHO STI guideline suggests using benzathine penicillin G 2.4 million units once intramuscularly over procaine penicillin G 1.2 million units 10–14 days intramuscularly.
Conditional recommendation, very low quality evidence
SUMMARY OF THE EVIDENCE
“Overall, there was very low quality evidence for outcomes after treatment of early syphilis. Evidence was gathered from 7 randomized and 18 non-randomized studies, each of which included one or two groups evaluating benzathine penicillin G, procaine penicillin, ceftriaxone, azithromycin and doxycycline (with or without tetracycline). Although not captured in published studies, most treatments today are based on historical and successful use of benzathine penicillin G and procaine penicillin.”
4.2. LATE SYPHILIS (INFECTION OF MORE THAN TWO YEARS’ DURATION WITHOUT EVIDENCE OF TREPONEMAL INFECTION)
ADULTS AND ADOLESCENTS
RECOMMENDATION 5
“In adults and adolescents with late syphilis or unknown stage of syphilis, the WHO STI guideline recommends benzathine penicillin G 2.4 million units intramuscularly once weekly for three consecutive weeks over no treatment.
Strong recommendation, very low quality evidence
RECOMMENDATION 6
In adults and adolescents with late syphilis or unknown stage of syphilis, the WHO STI guideline suggests benzathine penicillin G 2.4 million units intramuscularly once weekly for three consecutive weeks over procaine penicillin 1.2 million units once daily for 20 days.
Conditional recommendation, very low quality evidence
SUMMARY OF THE EVIDENCE
“Overall, the quality of the evidence was very low. Most studies typically include people with early or late syphilis and don’t distinguish between the stage of syphilis when reporting the results. However, one study included over 300 people diagnosed with late syphilis. It evaluated benzathine penicillin G 2.4 MU given once IM and azithromycin 2 g given once orally. Serological cure was low (33–39%); these doses are typically provided for early syphilis.”
“Because the benefits probably outweigh the harms, and because of the potential for resistance to azithromycin, greater cost and lack of historical data for azithromycin, benzathine penicillin G and procaine penicillin were suggested.”
https://www.ncbi.nlm.nih.gov/books/NBK384905/#_NBK384905_pubdet_
One other piece of key information that they forgot to tell us about was that the penicillin injections used as a treatment are highly toxic and can cause the exact same symptoms seen in syphilis and other diseases, and then some:
What side effects may I notice from receiving this medication?
Side effects that you should report to your doctor or health care professional as soon as possible:
allergic reactions like skin rash,
itching or hives,
swelling of the face, lips, or tongue
bloody or watery diarrhea
fever
redness, blistering, peeling or loosening of the skin, including inside the mouth
Side effects that usually do not require medical attention (report to your doctor or health care professional if they continue or are bothersome):
dizziness
drowsiness
headache
nausea
pain, redness or irritation at the site where injected
vomiting
This list may not describe all possible side effects.”
https://my.clevelandclinic.org/health/drugs/20943-penicillin-g-benzathine-injection
Sadly, these three injections for an imaginary stage of a non-specific and often absent disease set in motion the collapse of my loved one’s health. The decision to allow the treatment haunts me to this day and it will be something I will forever regret. The only silver lining is that this tragedy opened my eyes to the horrific lies that we have been sold for centuries. In order to ensure that future generations are not tricked by this ruse, let's explore how the stages of syphilis were created to fool the frightened into the toxic treatments.
For the greater part of its history, the symptoms of syphilis consisted of chancres, ulcers and boils reminiscent of leprosy. The biggest difference between the two was said to be in the mode of transmission, where syphilis was considered to be sexually transmitted while leprosy was not. As time passed, syphilis became known by many different names such as “the French disease,” “the Neapolitan disease,” “the German disease,” “the Russian disease,” ot even “the Christian” disease. It was also known as “the Great Pox” in an attempt to distinguish it from smallpox. However, no matter what name was given, the symptoms were indistinguishable from other diseases. Syphilis was regularly confused with not only leprosy but also chlamydia, gonorrhea, smallpox, measles, etc. This inability to distinguish syphilis from other diseases clinically earned syphilis another name as it became known as “the Great Imitator.” Thus, it can be seen that the symptoms associated with the disease were not specific and overlapped with many other conditions.
By the 18th century, there was a concentrated effort to try and separate non-specific symptoms into distinct diseases. Edward Jenner attempted to distinguish smallpox from cowpox and other ailments while William Heberden attempted to differentiate chickenpox from smallpox. These were all names for the same disease process used interchangeably depending on the physician and the part of the world they were in. At this time, it was also argued over whether syphilis and gonorrhea were separate diseases or were actually one and the same. In 1767, prominent surgeon John Hunter was said to have settled the argument when he inoculated a healthy subject with material from a patient with gonorrhea who then came down with symptoms of syphilis. Thus, both diseases were considered one and the same for the next 70 years. However, in 1837, French physician Philippe Ricord stated that he performed the exact same experiment as Hunter on 17 prisoners and claimed that his results showed that the two diseases were separate. From there, he went on to break syphilis into the distinct stages that we know it as today:
Case histories
Syphilis
From the mid-18th century, physicians and surgeons argued over whether syphilis and gonorrhoea were two different diseases, or two expressions of the same disease. In 1767 British surgeon John Hunter claimed to have proved, on the basis of an experiment in which he inoculated himself with gonorrhoea, that they were identical; he seems unwittingly to have used a needle also contaminated with syphilis. In 1837 the French–American physician Philippe Ricord repeated the experiment, not on himself but on 17 prisoners in Parisian jails, showing that gonorrhoea was a separate disease and not a symptom of syphilis. Ricord went on to describe three stages of syphilis: primary and secondary arose within weeks or months of infection, but tertiary syphilis might take a decade or more to develop after a period of latency. His student, the dermatologist Jean Alfred Fournier, showed that two apparently psychiatric disorders—general paresis of the insane, a severe form of dementia, and tabes dorsalis, a creeping blindness and paralysis—were symptoms of tertiary syphilis.”
https://doi.org/10.1016/S0140-6736(18)30833-X
Based on excerpts provided below from his work, Philippe Ricord went against the prevalent teachings of John Hunter by claiming that venereal diseases were caused by distinct entities. The biggest point of contention in separating syphilis and gonorrhea into distinct diseases was determining if the resulting sore was referred to as an ulcer or a chancre. If a sore was identified as an ulcer, this meant a diagnosis of gonorrhea. If the sore was identified as a chancre, this was given the label syphilis. Interestingly, Ricord stated that the specific entity causing syphilis was only an entity in the sense that hydrophobia (the fear of water) and snake venom (a poison) are entities. In other words, one “entity” was psychological distress and the other was a poison. He seemed to go against common thought that, once “cured,” syphilis could not be transmitted to another person. Ricord also stated that one could experience the same symptoms again but only if they came into contact with the pus or caught the disease from someone else. Looking at these as symptoms of detoxification, it makes sense that they would reappear if the person was still in need of cleansing. Instead of realizing that this process was not caused by any entity, Ricord assumed the individual was reinfected. He believed that having a general infection did not stop one from obtaining other ailments and infections. Thus, Ricord was attempting to make the case that, because someone who was diagnosed with gonorrhea could later be diagnosed with syphilis, and vice versa, these were not the same process but, instead, were diseases caused by different entities.
Ricord argued against those who noted that the symptoms associated with syphilis came after an initial bought of the symptoms of gonorrhea. He claimed that these cases were just misdiagnosed. He felt that the fact that these chancres could be found after sexual intercourse or after a mother breast fed her baby, that something must have passed between two people. Oddly, while he pointed out the role that friction plays in creating such sores, he maintained that this created the entry for the unseen entity, rather than being the cause of the sores themselves. Based upon the presumed difference of whether the sore was an ulcer or a chancre, Ricord separated syphilis into the main theoretical stages we see today, all without ever directly identifying the causative agent:
Philippe Ricord (1800-1889) Syphilographer
“Ricord soon acquired an international reputation through his captivating lectures, experimental studies of inoculation of the venereal virus, and clinical judgment of the ambulatory and bedridden. The identification of syphilis and gonorrhea as distinct diseases deviated from the respected teaching of John Hunter, who had not differentiated the venereal entities. By repeating Hunter's experiment of inoculation, Ricord identified the specific pathogenesis of the virus, separating virulent syphilis from nonvirulent blennorrhagia (gonorrhea) and dividing the clinical manifestations of lues into the three stages currently acceptable more than a century later—primary, secondary, and tertiary. These pertinent clinical deductions were presented in a monograph published in Paris in 1838 and translated into English in 1842.
Hence, according to the opponents of inoculation, must we not admit that when the pus of an ulcer produces certain symptoms constant in their form and development, and which present certain characteristic conditions, the ulcer, whose pus has been inoculated, was a chancre, and consequently that the necessary character, without which an ulcer cannot be called chancre, is to furnish a pus capable of being inoculated under the given conditions?
To most persons, who will examine with unprejudiced minds, it must be clear from the study of the phenomena of general contagion, and, as I have before said, from the constant and regular connexions between cause and effect, that the syphilitic diseases are ascribable to a specific agent or deleterious principle, which is only to be considered an entity in the same degree as the peculiar principle of hydrophobia, the venom of the viper, the specific cause of the small pox, &c. &c. &c.
Now, the incontestable existence of the venereal virus is proved by a peculiar property of a distinct morbid secretion, and therefore the pus furnished by certain syphilitic affections has the constant and regular property of reproducing a pus similar to itself.
I. A venereal affection already cured, or still existing at any period of its duration, does not prevent others being contracted, and the number of successive infections cannot be limited.
II. An individual actually infected, and under the influence only of primary symptoms in one region, never sees symptoms similar to the first developed in other parts of his system, except by a new contagion from contact with the pus of the first, or communicated by another individual.
III. Secondary symptoms, or general infection, never prevent the patient from contracting other primary affections.
IV. The frequency of constitutional syphilis bears no direct ratio to the number of primary symptoms developed at one time.
Do not the observations of former times combine with daily experience to corroborate the experiment of Hunter, which prove that one infection does not prevent a second; not only in the development of symptoms different in form and principle, but also of those which are owing to a cause of the same nature? Do we not often see patients who have a blenorrhoea contract a chancre by other sexual intercourse; or who have at first a chancre, and are attacked with gonorrhoea, after a new coition? I should think no candid person would attempt to deny so well known a fact. But the manner in which the symptoms following the first are produced, might be contested. Those who think there cannot be a primary infection without general symptoms, look upon all those which follow as in consequence of a first symptom, without the necessity of a new contagion. Thus they attribute distinct diseases, contracted at different times, to the same cause.
The most common means of propagating syphilis, is undoubtedly that by the sexual organs in the intercourse between the sexes; because the virus generally has its seat in these organs, and because they are always moist, and the epidermis which covers them is delicate and thin, the organs remain in contact, and friction renders absorption more easy. The organs of the mouth are often the propagators of the contagion by a lascivious kiss, by the application of the lips or tongue to some part of the mucous membrane, by suction of the breasts, and especially in suckling. If the mouth of an infant can infect a nurse, the breast of a nurse can infect a child. We confess our incredulity as to contagion by means of a seat of a privy or a chamber-pot, which no one had used for several hours; or a sponge not used since the previous day.
4. The symptoms of constitutional syphilis are not the consequence of blenorrhoea. In all the cases in which authors mention that it was an antecedent, the frequency of which precisely corresponds with that of masked chancres, (chancres larvés,) the diagnosis was not correct; the diseased surfaces not having been examined.
INOCULATION DISTINGUISHES PRIMARY FROM
SECONDARY SYMPTOMS
My clinical observations have led me to the following classification of the symptoms of syphilis.
1. Primary symptom, (accident primitif,) chancre from the direct action of the virus which it produces, and by means of which it propagates itself by contagion from a diseased to a healthy individual.
2. Successive symptoms, (accidents successifs,) or those which arise from contiguity of tissue, or by simple extension of the first local symptom, as new chancres; simple inflammatory, or virulent abscesses, or simple or virulent adenitis, &c.
3. Secondary symptoms, or symptoms of general infection, in which the virus has undergone a modification and produced the syphilitic temperament; symptoms appearing on the skin, the mucous membranes, the eyes, testicles, &c, and seldom happening before the first two weeks of the duration of the primary affection, chancre; but generally after the fourth, sixth, eighth, or even much later; not capable of inoculating.
4. Tertiary symptoms (accidents tertiaries,) occurring at indefinite periods, but generally long after the cessation of the primary affection; not appearing in most subjects until after secondary symptoms have occurred, . . . Under the head of tertiary affections, we must place nodes, deep seated tubercles, tubercles of the cellular tissue, periostoses, exostoses, caries, necrosis, syphilitic tubercles of the brain.”
https://jamanetwork.com/journals/jama/article-abstract/351224

This next source provides even more detail on Ricord and his methods. It is stated that prior to Ricord’s research, many “traditionalists” believed that all venereal diseases were the same. Some traditionalists felt that venereal symptoms should be treated with mercury while others felt that this was too poisonous and preferred sweating and bloodletting to help detoxify the body. Ricord himself had no background with venereal disease but decided to go against the prevalent thoughts in order to tackle the issue himself. He campaigned for the reintroduction of vaginal speculum and created his own instrument to open the vagina in order to find unsuspected vaginal chancres. However, it is said that his second investigative invention, the autoinoculation, led to unfortunate results. This is a procedure where cells are removed from the body, treated and medically changed, and then re-inserted back into the body. Ricord's method consisted of taking material from a genital ulcer, urethral discharge or draining lymph node and then re-inserting this back into the patient's own thigh. He would then cover it with a watch glass and observe it daily for the development of lesions. This method led to erroneous results as it was later determined that many of the venereal ulcers Ricord utilized were, in fact, non-syphilitic and were most likely chancroid.
Oddly enough, despite his errors, Ricord accused other physicians of “errors, ignorance and special pleading” while championing his own results as the truth. Ricord had set out to establish both a specific cause of syphilis as well as to distinguish diseases that were similar to each other. He obviously failed with his first endeavor as the T. pallidum bacterium, which became associated with syphilis, was not discovered for another 68 years, and even that remains unproven. He also failed to adequately distinguish similar diseases as there is confusion to this day. It is said that Ricord believed that the inoculation of any ulcer will always reproduce the same ulcer. However, he admitted that the ulcer may not form depending on the predisposition of the individual and the area affected. In other words, as we see with many in the sciences, he held completely contradicting beliefs. As he could not reproduce the same chancres from patients suffering from “secondary syphilis,” Ricord concluded that this stage was not contagious, going against the modern interpretation. He was also unsuccessful in recreating the same disease in animals and due to this failure, concluded that it was solely a human pathogen.
Ricord expressed that if the chancre was either cauterized or excised, secondary syphilis would not occur, thus seemingly negating the current use of penicillin as a “cure.” Like the rest of the medical professionals of the day, Ricord also recommended the use of mercury as a treatment. Due to Ricord's belief that secondary syphilis was not contagious, he had many disagreements with his colleagues. However, Ricord would not back down in his belief and when they would point to chancres reminiscent of primary syphilis in those said to be encountering secondary syphilis, Ricord would brush their observations aside and say it was confusion as the chancres looked similar. They also criticized his autoinoculation procedure, stating that Ricord should test on healthy subjects rather than using the same subject for experimentation, but Ricord would not budge. Thus, it is clear that Ricord was a stubborn man who refused to acknowledge findings that contradicted his own and, like any good pseudoscientist, found ways to explain them away. In the end, it is stated that, while the stages of syphilis were established, the causative agent remained unknown, there was no experimental animal model to recreate the disease, and the methods used for diagnosis and treatment were unsatisfactory. Thus, we can ask ourselves, what really did Ricord do other than create a hypothetical model?
Eminent venereologists. 3. Philippe Ricord
“At the time of Ricord's appointment venereology was in a state of chaos, for which John Hunter was largely responsible. Many traditionalists still believed, like him, that all genital ulcers and discharges were due to syphilis, and should be treated with mercury. Others thought that mercury was poisonous, and advocated the ancient treatments of bleeding and sweating. Inevitably, charlatans and quacks abounded. Ricord had no background in venereology, but he decided to think carefully about what he saw and keep an open mind while he formulated his ideas. He was struck by the inadequate diagnostic techniques of the day, particularly for women. Prostitutes, for example, were declared "infected" or "not infected" by simple inspection of the vulva and palpation of the vagina. Ricord called this "blindfold diagnosis"; he mounted a campaign for the reintroduction of the vaginal speculum and devised a bivalve instrument himself, with which he was able to demonstrate previously unsuspected vaginal and cervical chancres. It is said that a splendid ivory and gold model was made for the exclusive use of the Empress Eugenie. His second diagnostic aid, autoinoculation, was to have uunfortunate results. The inoculation of material from genital lesions and discharges into normal subjects was an experimental method which had been in use for many years, and had been enthusiastically advocated by Hunter, Wallace and many others. Ricord was firmly convinced that it was wrong to inoculate healthy people with diseases whose consequences were unpredictable. His technique was to inoculate material from a genital ulcer, urethral discharge or draining lymph node into the patient's own thigh, cover it with a watch glass and observe it daily for the development of lesions. Between 1831 and 1837 Ricord performed more than 2500 of these inoculations.
In 1838 he published "Traite pratique des maladies venenennes, in which he set out his ideas in detail - ideas which actually changed very little during the rest of his long life. He began by accusing most previous workers on the inoculation of syphilis of error, ignorance, special pleading and bad faith, contrasting these with his own researches which, according to him, were pursued without preconceived notions and with the object of discovering the truth. His aims were: (1) to prove the existence of a specific cause of syphilitic diseases, (2) to distinguish between diseases which resembled each other, (3) to establish the differences between primary and generalised syphilitic infection, (4) to improve treatment and, if possible, prophylaxis, and (5) to consider public health and legal aspects of syphilis. In the first section of the book Ricord reviewed the literature, quoting Bell and Hernandez with approval, then expressed his own ideas on the inoculation question: (1) An ulcerated chancre, and its consequent bubo, will always reproduce a chancre when reinoculated; so will the pustule caused by the inoculation. (2) Induration of a chancre may or may not occur, depending on individual "predisposition" and the part affected; induration usually indicates that a generalised infection is likely to follow. (3) Inoculation of material from the ulcers of secondary syphilis will not induce a chancre. (4) Inoculation of the pus of blenorragia [gonorrhoea] also gives negative results. Ricord concluded that syphilis had one specific cause, that gonorrhoea, balanitis and condylomas were not due to syphilis, and that secondary syphilis was not infectious. He advised that the reinoculation technique should be used to prove that a venereal ulcer was syphilitic, the diagnosis depending on the prompt development of a pustule at the inoculated site; non-syphilitic ulcers gave negative results. In "serious and urgent circumstances" the test could be used to decide whether marital intercourse was safe.
The second part of the book provided clinical and experimental data, including nearly 200 case reports, to substantiate these ideas. Ricord clearly recognised the primary, secondary and tertiary stages of syphilis, although he thought that the primary lesion begins as a pustule, with no incubation period. Attempted animal inoculations were unsuccessful and he concluded that syphilis is specific to humans. The third part of the book was concerned with therapy. He believed that secondary syphilis never develops if the chancre is destroyed by cautery or excision in the first five days. Like everyone writing about venereal disease at the time, he included a long section on the use of mercury. His ideas on this subject were not very clear, but he certainly recommended it for secondary or late syphilis. He gave details of the treatment modalities in use at the Midi, and discussed the prevention of infection, emphasising the importance of local hygiene, and recommending the examination of prostitutes with the speculum every three days.
The historical importance of Ricord's Traite lies in the conclusive separation of gonorrhoea from syphilis, and in the orderly arrangement of the stages of syphilis. His autoinoculation technique, although claimed by him as "the sole rigorous method available" was in fact no such thing; its conclusions were erroneous, and were to lead him into a bitter and eventually humiliating controversy. Today, it is clear that many of the venereal ulcers he dealt with were non-syphilitic, and probably due to chancroid. But these reservations did not apply in the 1830s; the Traite received immediate acclaim, it was translated into German, Dutch, English and Italian, and won Ricord a gold medal from the French Academy of Sciences. He was thought to have brought order out of chaos, and he soon became established as a leading syphilologist, and the Midi as a major centre.”
Ricord was sure, mostly because of his inoculation experiments, that the lesions of secondary syphilis were not contagious. Some doctors, including his junior colleague at the Midi, Vidal de Cassis, did not share this view; they thought that he had become too dependent on his inoculation technique, and believed on clinical grounds that "secondary contagion" was possible. Ricord refused to give way, saying that it was always possible to mistake the ulcers of secondary syphilis (which were not contagious) for those of primary syphilis (which were contagious). It was pointed out that autoinoculation was not the technique to settle the problem, and that inoculation of a healthy volunteer would be better. This had been done by William Wallace,' apparently successfully, but Ricord said that it was unethical, and refused to consider it. Vidal did not share these scruples, and in 1851 inoculated a pharmacy student with material from a pustule on the breast of a patient with secondary syphilis, inducing a typical primary chancre.' Ricord criticised his colleague on ethical grounds, suggested that Vidal's source lesion was a misdiagnosed primary chancre, and continued to hold his ground. Vidal, who was in a difficult situation, had to content himself with the remark: "Hunter was encased in his doctrines. He had unswerving convictions, just like Ricord, for I believe my colleague is of the doctrinal family of Hunter."
“During the first half of the nineteenth century careful clinical observations, supplemented by the use of inoculations, made it possible to separate syphilis, gonorrhoea and chancroid, to clarify the natural history of syphilis and to begin the study of congenital syphilis. But the aetiology of these diseases was unknown, no experimental animal had been found, there were no satisfactory diagnostic tests and treatment was unsatisfactory. In the end, clinical observation had to give way to laboratory methods. It is sometimes said that Ricord's death marked the end of an era, but the era had effectively ended twenty years earlier with Neisser's discovery of the gonococcus. From then on, advances in venereology were to come from the laboratory rather than the consulting room, and leadership in medicine, centred in France for the previous half century, was to move across the Rhine.”
Interestingly, after the publication of his work, there were still many people in disagreement with Ricord and the separation of a disease called syphilis from other diseases. In 1903, Professor Ottomar Rosenbach, a bacteriologist, wrote a book going against the modern interpretation of syphilis. He argued that there was no increase in syphilis cases and that this “increase” was nothing more than the result of diagnostic measures labeling many unrelated conditions under the syphilis umbrella. He was against the act of tracing many conditions to a supposed syphilitic origin and then attributing it as the cause of said symptoms. He stated that the presence of a bacterium alone was not evidence that it was the causative agent of the symptoms, or lack thereof, associated with it.
Albert Neisser, director of the dermatological clinic in Breslau since 1882, was another of Ricord’s detractors. This was due to the attempts by dermatologists to catalogue the various eruptions and skin conditions that were being associated with the secondary and tertiary stages. Neisser declined a chair position offered to him as he felt that it was impossible to teach students what a syphilitic lesion was when syphilis was now claimed to mimic them all:
Spirochaetes Serology And Salvarsan
“It may be worthwhile to examine the views of one particular dissident who questioned the aetiological status of the pale spirochaete: Professor Ottomar Rosenbach, a colourful critic of bacteriology and a staunch defender of the virtues of clinical medicine. In his book Das Problem der Syphilis (1903, second edition 1906) he had already launched a full-scale attack on modern ideas about syphilis. Rosenbach dissociated himself from the widely held alarmist view that the incidence of syphilis had increased dramatically during the previous decades. In his opinion, this impression was largely the result of a diagnostic fashion: "for one hardly meets a case history of myocardial affection, arteriosclerosis, or nervous disease, in which lues is not adduced as aetiology". Rosenbach did not recognize the syphilitic nature of neurological disorders like tabes and general paresis or of cardiovascular affections like aortic aneurysm. He opposed what he called the "monistic way of thinking", which attempted to trace various kinds of affections back to a syphilitic origin and syphilis itself to a tangible microbial agent. Rosenbach accused the adherents of the pale spirochaete of taking insufficient care to avoid the vicious circle: "Because one considers the carrier of the spirochaetes to be luetic, one is naturally tempted to attribute to the microbes found with him the character of Spirochaeta pallida [...]". The vicious circle was also supposed to turn the other way around: "The problem is to establish the causative agent of lues, and it is not allowed, if one considers Spirochaeta pallida as such, to assume as proved what has yet to be proved, i.e. to take the presence of spirochaetes as positive evidence for the existence of a luetic infection [...]". Rosenbach therefore formulated the following methodological requirement: "One should, without knowing the clinical diagnosis, consequently without any subjective prejudice, attempt to determine the parasites in all tissues and lesions in which spirochaetes are to be found, or, even better, have them determined by a person uninformed about the nature of the disease case".
“Traditionally, syphilology is intimately linked with dermatology. An earlier generation of clinical investigators had patiently described and catalogued all the various cutaneous manifestations which syphilis shows in its 'secondary' and 'tertiary' stages (a terminology in accordance with Philippe Ricord's [1800-1889] division of the natural course of the disease into three stages). Since then medical students had to be thoroughly trained in distinguishing syphilitic eruptions from closely resembling non-syphilitic skin diseases. For Albert Neisser, director of the dermatological clinic in Breslau since 1882, this circumstance provided a motive to decline the vacant dermatology chair in Berlin offered to him, as he explained in 1890 in a letter to the all-powerful Prussian official Friedrich Althoff:
"Of the one hundred questions, which force themselves on the specialists or the practical physicians working in the relevant area during their daily practice, at least ninety turn on the decision: syphilis or no syphilis? The fact that syphilis mimicks nearly all known socalled idiopathic diseases implies that in any instance of cutaneous eruption first of all the differential diagnosis with respect to syphilis has to be made and examined in depth. A separation of the two subjects in a syphilis-clinic and a skin-diseases clinic [as corresponded to the situation in Berlin - HvdB], however, makes it impossible for the lecturer to teach the students precisely that which he should impart on them as the first and most important thing."
Another source offers that Ricord himself understood that his methods were attacked. Even after he published his work, there was no agreement on what syphilis was. This debate was said to last long after the publishing of Ricord's treaties and that the interpretation of what syphilis was changed regularly. Thus, Ricord's evidence and his hypothetical model of the stages of the disease did not end the debate between the traditionalists and those who believed otherwise:
On the Origins of the Modern Concept of Syphilis
Contemporary support for Ricord?
While history records that Ricord, not Bell, was the first to discern syphilis and gonorrhoea, an interesting question to ask now is: to what extent was Ricord’s theory of the dualist nature of syphilis accepted by his peers? Ricord himself mentioned that his empirical methods were “vigorously attacked.” In 1852, a decade after the English translation of his Traité, there was still no agreement over the nature of syphilis in London. One physician, while acknowledging his French colleague as “genius”, nevertheless remarked,
The common result of the contact of the syphilitic poison with the mucous membrane of a sound person, is the production of an ulcer; but I believe, also, that its effect may, in some instances, be a purulent discharge, constituting a common Blennorrhoea, or Gonorrhoea. In these cases I further believe, and have satisfied myself of the fact, that constitutional syphilis will follow with as much certainty as if it were preceded by a chancre.
From this, it can be seen that debate about the nature of syphilis endured long after Ricord’s publication.
Historical understandings of syphilis have not remained static. Arrizabalaga wrote that since the publication of Ricord’s work, the concept of syphilis was constantly reshaped until it reached its current scientific state today. Despite historians and scientific writers emphasising Ricord as a pioneer in syphilology, it is clear that he was but one contributor in a debate that had endured throughout the preceding century. While modern historians recognise that Ricord’s conception of syphilis resembled modern understandings of the disease, particularly with reference to his epistemological methodology (including the use of experiments, and the use of a speculum), he himself recognised the significance of Bell’s work to his own views. Ricord’s work can be seen then as an important contribution to an on-going debate that did much to support the dualist theory. However, it did not end the debate. Ricord was by no means the first physician to marshal powerful arguments and evidence in support of the dualist position.”

What we are left with is the unsuccessful differentiation by Ricord of ulcers and chancres shared between supposedly different venereal diseases and the creation of a hypothetical framework for how this disease apparently progressed. However, one thing that was seemingly unaccounted for by Ricord, in the development of these stages and the symptoms associated with them, was the toxic side effects created by the poisonous treatments used to combat the disease. For most of its history, the main method utilized to “cure” syphilis was the use of mercury, either as an ointment, as an injection, or taken orally. This led to horrifying symptoms said to be worse than the disease itself, such as ulcers, fragile bones, and even death:
“By the 17th century, mercury had become the standard European therapeutic for this new plague. Mercury could be taken orally, injected into the urethra with a syringe, or made into an unguent and rubbed onto the skin. This cure could be as fearsome as the disease, provoking uncontrollable salivation along with ulcers, loose teeth, fragile bones, and nerve damage in an attempt to rid the body of corrupted humours.”
https://doi.org/10.1016/S0140-6736(18)30833-X
It is well-known that mercury is a neurotoxin that has devastating impacts on the brain. It accumulates in the body and can cause memory loss and other neurological disorders:
Mercury poisoning through intravenous administration
“Chronic metallic mercury intoxication may induce symptoms from the central nervous system including tremors, delusions, parkinsonism, memory loss, and neurocognitive disorders. The correlation between the declining neurological function and the increasing exposure has been reported. Severe exposure may result in a lasting effect on nervous system and brain function.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5704834/

If one was being honest, they would see that the use of mercury as a treatment caused many of the long-term neurological symptoms syphilis patients experienced. However, instead of admitting this, these symptoms were lumped into the tertiary stage and given the label neurosyphilis. While the use of mercury as a treatment alone should be enough to question the many symptoms thrown under the syphilis umbrella, it was eventually phased out as a treatment for a drug call Salvarsan. This drug was created by Paul Ehrlich (of antibody fame) and was derived from arsenic, a chemical regularly used to murder people. This drug, also known as 606, was taken by healthy people with no symptoms in order to ensure that they would not get the disease. It was essentially one of the first chemotherapies to be used. The drug was dangerous and had many detractors calling for it to be discontinued due to side effects including rashes, liver damage, and risks of life and limb. Thus, once again we can see that the treatments caused the very symptoms of disease blamed on the bacterium which was never scientifically proven as the cause:
The Salvarsan Wars
“BEFORE 1910 THE ONLY TREATMENT AVAILABLE FOR SYPHILIS was about as terrible as the disease itself: the liquid metal mercury, which could cause death or organ damage. So when the first clinically tested syphilis agent debuted 100 years ago, it quickly became the most prescribed drug in the world. “People who…have shown no evidences whatever of disease…have been begging for a dose of ‘606,’ just to make ‘perfectly sure,’ ” one U.S. physician reported.
Behind 606 was the German physician Paul Ehrlich, who had shared a Nobel Prize for his work in immunology two years before. Yet little did this kindly scientist know that he would soon be embroiled in controversy.
Ehrlich’s assistant, Japanese bacteriologist Sahachiro Hata, had found a way to infect rabbits with the syphilis-causing bacteriumTreponema pallidum, and, as possible cures, the duo tested arsenical compounds that Ehrlich and chemist Alfred Bertheim had developed. When Hata injected the 606th substance, arsphenamine, intravenously into live animals, it killed the syphilis bacterium—but not the rabbits. By September 1910, 606 was on the market under the brand name Salvarsan.
The drug put into action two ideas that Ehrlich had conceived earlier: chemotherapy, a term he coined for “curing organisms infected by certain parasites in such a way that the parasites are exterminated within the living organism…by the use of substances which have had their origin in the chemist’s retort”; and “the magic bullet,” meaning drugs that home in on disease-causing microorganisms.
This magic bullet was difficult to administer, however, and the side effects—rashes, liver damage, and risks of life and limb, literally—prompted some physicians to denounce 606. In what historians have dubbed the Salvarsan Wars, Ehrlich and Hata were vilified for profiting from what their detractors called a dangerous drug, even claiming that Frankfurt Hospital had forced prostitutes to undergo Salvarsan treatments. Ehrlich was accused of criminal negligence, though he was eventually exonerated.
https://protomag.com/infectious-disease/paul-ehrlich-and-the-salvarsan-wars/
While it would be easy to go on and on about Ricord's ruse, hopefully the examples from the above sources provides a clear enough picture that the same symptoms of disease were separated into distinct diseases based on the flimsiest of differences. Ricord created a hypothetical model for stages of a disease process that was reflective of the treatments used as a “cure.” If one had a chancre after sex, they were treated with mercury rather than allowing the body to heal naturally. The effects of this poisoning would come out as secondary detoxification symptoms as the body attempted to flush the mercury out. More severe symptoms created by the continued use of mercury, such as neurological disorders and deformed bones, were placed into the syphilis mold.
As it became recognized that the use of mercury was too toxic, another drug was created from an even deadlier compound in arsenic. This poison would cause rashes of all kinds and damage the internal organs. It caused people to lose both their limbs and their lives until penicillin came around, pushing the arsenic drug aside due to its toxicity. However, that did not stop the symptoms associated with its use from being added to the syphilis brand.
Now, we have a treatment based upon low quality evidence that can cause the exact same symptoms associated with the disease it is supposed to cure which can lead to a total collapse of one’s health. When will penicillin be discarded in favor of the next “less lethal cure?” What new symptoms will fall into the expanding pathological picture of syphilis? Sadly, just as we were tricked into treatment for my relative based upon the fear that a bacterium was waiting in the wings for the right moment to strike, others will be subjected to this same propaganda and receive the same toxic treatment. This perpetuates a cycle of fear and ignorance over a centuries long fraud that has remained hidden for far too long. In order to destroy Ricord's ruse, we must realize that the disease and its stages are a cover-up for the toxic effects of its treatments. If this happens, maybe we can finally end this syphilis scam once and for all.

https://whatreallymakesyouill.com/the-real-tragedy-of-tuskegee/
took a very entertaining look at the WHO'S criminal "pandemic" treaty.
Steve Falconer, of Spacebusters fame and well-known for his excellent germ theory-busting documentaries, was in the Patrick Henningsen show debunking gain of function.
https://odysee.com/@spacebusters:c9/Gain-of-Fiction-Lab-Leak-BS:4
has a very motivational and uplifting look at the “No Virus" International team around the world that is spreading the word that the emperor has no clothes.
I used to "know" and "believe" that contagious disease through microbes was real.
Now that I have doubts, I see so many people who "know" and "believe" like I did. In some cases, their lives revolve around this idea, because their chronic disease or disbility has become identical to their personality. They are their disease.
In other cases, they are sure because it is their profession.
But they become angry when they hear other person expressing doubts. Having doubts means, for them, that the doubter denies disease, pain, suffering. That's a bad way to reason, but they don't care about logic.
Frauds would be more difficult to pull if people knew more about logic, and about their emotions.
I am now curious about the tuskegee experiments. They claim these black men were infected with syphilis and left untreated, resulting in full blown disease and transmission to their spouses.