


The Syphilis Scam: Imitation Game
The sincerest form of fakery.


Throughout human history, those who have suffered noticeable signs of disease have been treated as outcasts and pariahs. This was most famously seen with those who suffered from the condition known as leprosy. These unfortunate souls, who primarily lived in poor, unsanitary conditions, were often covered in ulcers, boils, and crustules all over their bodies. They were regularly disfigured from the scarring caused by these eruptions of the skin. People feared that this was a condition that was divinely ordained upon the individual as a punishment for some sin and it was feared that this state was highly contagious. Based upon these fears, the victims were often shunned by families, friends, and their own community. They were forced to live either alone in isolation far away from civilization or in leper colonies with groups of people suffering from the same condition.
As time progressed and these symptoms of disease did not disappear, other names and explanations were given for the continued appearance of the disease. In the 16th century, these symptoms were rebranded as a new condition that was sexually transmitted and eventually given the name syphilis. This led to many of the victims who suffered these same lesions to be considered impure. Blame for the disease was placed primarily on the women and the poor. As with leprosy, victims of the disease were treated as social outcasts, no longer fit to remain in the public sphere due to the morality of the act that was said to bring about their ailment.
In modern times, we have seen this same fear and impure stigma placed upon those who were suffering similar symptoms and then labeled with an HIV diagnosis starting in the 1980's. Many saw this as a punishment for the gay and/or intravenous drug abusing lifestyle. Once again, the poor and those who were engaged in sexual acts were targeted as the victims of the disease and shunned by society. Those with the HIV/AIDS label were, in many cases, restricted in terms of being able to travel to certain countries as well as being employed in certain jobs.

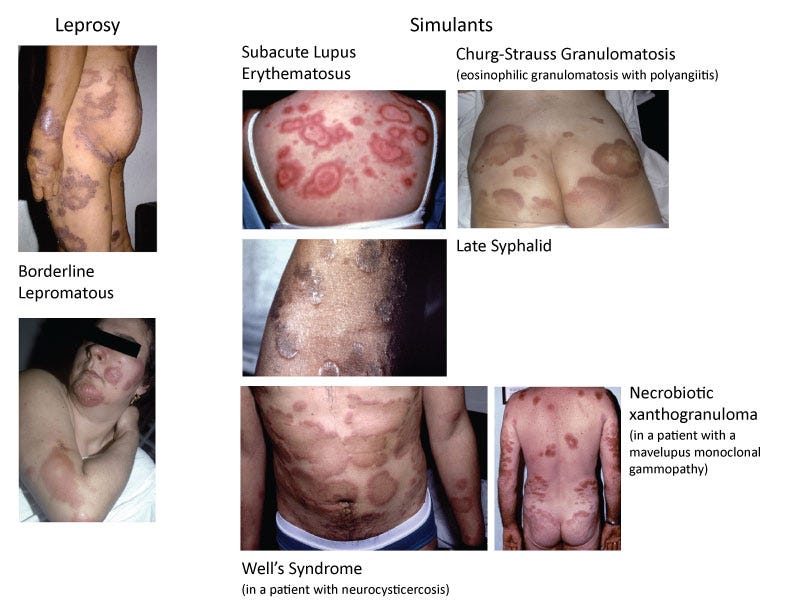
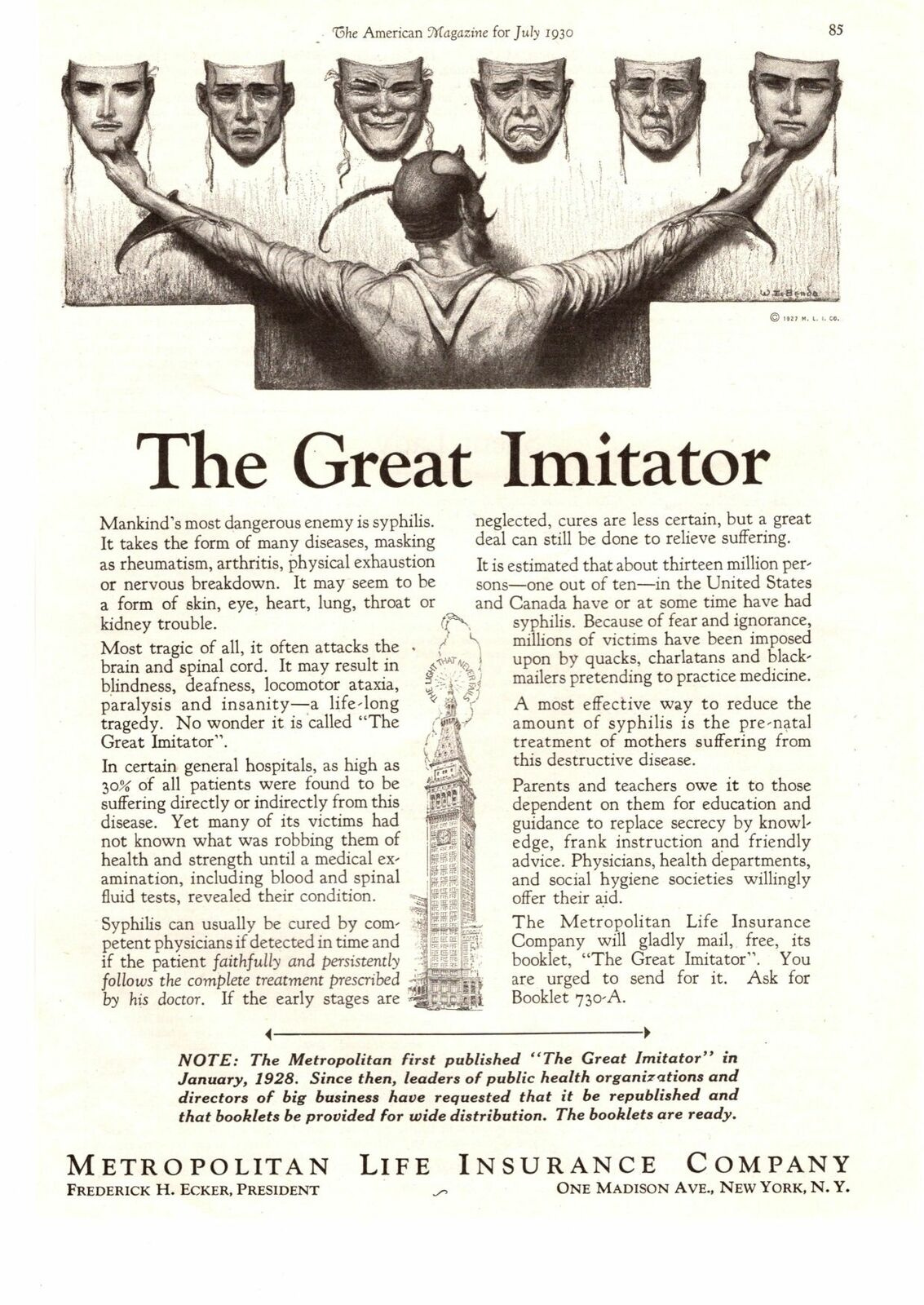
The above examples are of diseases that deal with illness and eruptions of the skin that are used to stigmatize certain groups of people. Both leprosy and AIDS are connected to syphilis as they are said to share many of the same signs and symptoms with the disease known as “the Great Pox.” They have been regularly confused for syphilis at the time of diagnosis and vice versa. However, while these conditions are the focus of this article, they are not the only conditions that are indistinguishable from syphilis. Throughout history, syphilis became known by the monikers “the great imitator” or “the great mimicker” as seemingly every symptom of disease became associated with the name at some point in time. As I shared in my last article, many of these symptoms can be traced back to the toxic treatments that were used as a “cure” such as mercury and arsenic. Once a presumed bacterium became identified as the cause, any symptoms a person experienced where this bacterium was identified, were also placed under the syphilis brand. It was a clever way to reframe a healing process into a contagious illness to wage war against. Yet, when one looks into the history of these diseases, it is clear that they are all stages of the same process that have been given different monikers based upon the time period that they were “discovered” in. Let's explore the connection that the symptoms identified as syphilis share with leprosy and AIDS and see what we can unveil about “the great imitators.”
“He who knows syphilis, knows medicine”
Sir William Osler
Syphilis and Leprosy
Throughout much of history, syphilis and leprosy were intimately connected as they shared the exact same symptoms of disease as well as the same “cures.” They were commonly mistaken for one another, and the victims were often stigmatized in the same manner. Was this just a coincidental case of two similar conditions presenting with the same symptoms or a case of mistaken identity? In order to examine this relationship between these diseases further, let's take a look at a few sources and see what we can uncover.
This first source is from a 2013 paper which examined the origins of syphilis. The main argument used as evidence that syphilis and leprosy were distinct diseases was that syphilis was considered sexually transmitted and that it could be given to babies upon birth, while leprosy was said not to be acquired in this manner. Obviously, these two stipulations would not be proof of separate etiological agents, only that the differing characteristics were used to assign a certain name to the same symptoms of disease based upon subjective criteria. In historical descriptions, the symptoms of leprosy, gout, palsy, and apoplexy were all said to stem from cases of syphilis. Early physicians did not distinguish between leprosy, gonorrhea, and syphilis as they were considered one and the same. However, recently, researchers have been going back to historical artwork and documents in order to start claiming that syphilis symptoms were mistaken as leprosy in order to make it appear as if the disease has been around longer. This does nothing but blur the lines between these supposedly distinct diseases even more. It is even noted that as France and Germany abolished their leprosy colonies, this created the appearance of syphilis epidemics as the lepers became more visible in society. As syphilis cases began to become more widely diagnosed, leprosy cases started falling, even though clinicians could not differentiate the two:
On the Origins of the Modern Concept of Syphilis
3.4 Identifying syphilis
“The symptoms of syphilis were historically identified with a number of unrelated diseases. As explained in Chapter Two, the symptoms resemble those of many other diseases. Historically, it was frequently confused with leprosy. Leprosy had outward symptoms broadly similar to a syphilis infection, but was transmitted neither sexually nor congenitally. Ulrich von Hutten presented an insight into how the French disease was understood in the sixteenth century:
Sometimes the Disease transforms itself into the Gout; at others, into a Palsy and Apoplexy, and infecteth many also with a Leprosy; for it is thought these Diseases are Neighbours each to the other, by reason of some Affinity there appears between them; those who are seized with the Pox, frequently becoming Lepers, and through the Acuteness of the Pain, Men will shake and quiver as in a Fever.
The puzzle that syphilis presented to early modern writers is clearly conveyed by von Hutten describing how the pox can become leprous.
Crosby placed culpability for this error on the notion that early medical knowledge did not differentiate between syphilis, gonorrhoea, and leprosy, and thus physicians were inclined to group similar symptoms or suspected modes of transmission as like diseases. Frequently referred to as a venereal disease, Barker et al. cite references to ‘leper whores’, ‘hereditary leprosy’, and medieval descriptions of genital lesions indicating that symptoms of syphilis were being attributed to leprosy. Recently, Old Testament accounts of leprous symptoms have been reassessed as symptoms of syphilis, the former a result of a mistranslation, according to Barker’s team. They refer to Deuteronomy (28:27-8) writing that “Moses described punishment for disobedience as manifesting “emerods”, scabs, itches that cannot be healed, madness, and blindness”; likewise, Job’s symptoms of a genital lesion, body-covering boils, and failing sight are now reputed to be signs of syphilis, and not leprosy as previously thought (Job 16, 19, 30).
Understandings of leprosy and syphilis remained closely entwined throughout the Middle Ages. In 1490 and 1505, Pope Innocent VIII abolished all leprosaria, resulting in thousands of sufferers returning to their homes. Prior to their abolition, France and Germany had an estimated 10,000 leprosy communities, while there were approximately 200 in the British Isles between the thirteenth and fourteenth centuries. Baker et al. emphasise that the average leprosy home catered for around ten people, creating a sizeable influx of sufferers back into communities. With physicians noting the stark similarities between these diseases, increases in the visibility leprosy with these abolitions may account for early “syphilis” epidemics during this period. Both Baker et al. and Eatough also make the point that as diagnoses of the “French Disease” became more widespread, diagnoses of “leprosy” became less common. In terms of medieval medical knowledge, this is interesting because Morbus gallicus, the French Disease, embraced a wider range of symptoms than what is characteristic of syphilis today. This suggests that the terms either incorporated other diseases or that the causative bacterium has since evolved.”
Both of these diseases have been regularly confused for one another at the time of diagnosis. This can be seen in articles from the late 1800's. Sir William James Moore, an honorary physician of the Queen and a Viceroy to India, believed that leprosy and syphilis were one and the same. In an August 1890 article in The Standard, he laid out various reasons for why he believed that leprosy was an inherited form of syphilis. He felt that this condition was acquired when one was in a constitution or temperament with which they are unacquainted, and that this was aided by a favorable environment. A Lancet editorial in response to Moore agreed that the diseases resemble each other while the Editor of the Hospital Gazette stated that leprosy was an exaggerated form of syphilis. Moore went through the objections of associating these diseases as the same and rebutted each one:
As with leprosy, mercury did not always “cure” syphilis and non-mercurial treatments were forcibly applied in the past.
Both conditions are associated with nervous system trauma.
The lesions of both could be severe.
Despite subtle distinctions of the sores, they are regularly confused.
The diseases have similar periods where the symptoms subside but can return at a later time.
The bacilli associated with the diseases are nearly identical (along with those seen in cases of tuberculosis).
While considered a newer disease than leprosy, syphilis may have been mistaken for leprosy in historical accounts due to the identical symptoms.
Both can result in acute febrile eruptions.
Hoarseness and nasal voice, destruction of the palate and nasal bones, and nervous affections are common to both illnesses.
The sores can not be differentially distinguished from one another.
It was common to refer to doubtful cases as “syphilitic leprosy,” "leproid " or "syphiloid.”
Cause of Leprosy
“Briefly, my views are as follows: That leprosy is a phase of inherited syphilis, which like other inherited taints, is partial in its distribution, and may not develop in one generation, although it may do so in the next; the development being determined by some condition of constitution or temperament with which we are unacquainted, aided by favourable environment. That, when developed, leprosy is capable of being conveyed by leprous matter coming into contact with a healthy one, or abrasion of the skin. But the connection of leprosy and syphilis as shadowed above, does not meet with general credence. For instance, a Lancet editorial said, "It is au old question that he (Sir W. Moore) has revived. . . . Now-a-days we think we know a little more about intimate pathology. ... At any rate we seek for the differences between diseases rather than confound those which are superficially alike. There is no doubt at all that syphilis and leprosy do closely resemble one another. . . . But this may mean nothing more than that they both belong to a similar class of morbid suites, that they are akin but not identical." On other hand, the Editor of the Hospital Gazette, agreeing with me, said “In opposition to the views of most of our contemporaries we have maintained that leprosy is an exaggerated form of syphilis." Now there are no class better qualified to give opinions on the matter than medical officers practising in India. I make this communication, therefore, with the view of eliciting opinions on the subject, and I am quite ready to alter my views, should sufficient reason be afforded.”
“I now come to the connection of syphilis and leprosy. Reasons as follows have been advanced against this view. (1) It has been stated that leprosy is not contagious like syphilis. But evidence has been adduced showing communication from contact. (2) It has been said that mercury does not cure leprosy. But mercury does not always cure syphilis, and it is not so very long back that the non-mercurial treatment of syphilis was forcibly advocated. (3) It is said that local loss of insensibility and enlargement of nerve trunks are not characteristic ot syphilis. But syphilitic affections of the nervous systems are sufficiently common. We have heard of paralysis of the cranial nerves, of atrophy of the optic nerves, and of fusiform neuritis in connection with syphilis! (4) The local ulcerations of leprosy are of a more severe character. Those who remember the ulcerations of syphilis forty years ago, may be inclined to doubt this. For destructions of the nose and palate, necrosis of the skull, aud other bones, extensive "bad legs" were not quite so uncommon as they are now! (5) Syphilitic skin patches are rounder than leprosy patches, the leprosy tubercles do not soften so rapidly, and do not form crusts. But notwithstanding these subtle distinctions, the one malady has been, may be, and will be, mistaken for the other, as in some forms and stages they are so much alike. (6) The absence of the periods of inactivity in leprosy which occur in syphilis. This may be denied. Leprosy often remains stationary for an indefinite period. Under good diet, oils, and good sauitary surroundings, the cachectic leper often becomes a robust leper; ulcers healing and recovery appearing in prospect. There are persons who have a minor degree of leprosy for years, just as there are those who have a minor degree of syphilis. (7) A distinctive bacillus. The leprosy bacilli are described as fine rods with pointed ends. The syphillis bacilli as rods with slightly thickened ends. And it is said the peculiarities both show in their mode of staining are shared with tubercle bacilli. It is very evident that the bacilli of tubercle leprosy and syphilis are very much alike, perhaps the same. It is not therefore surprising if they are found associated with similar diseases. (8) Hereditary syphilis comes on quicker after birth than leprosy. This is often the case, but not always. A child, afterwards developing leprosy, is born apparently healthy. And a child who afterwards develops syphilis may be born apparently healthy and remain so for a long time. (9) It has been advanced, that leprosy has existed from time immemorial, while syphilis is a comparatively recent disease. This may be questioned. There appears to be an allusion to syphilis in the 3rd Book of Moses; and it is very likely that as at a much later era in England syphilis and many other sores were regarded as leprosy. Shakespears speaks of the "leproaity of disloyalty," and Bacon of the “crudities, impurities and leprosities of metals"-showing that leprous and analagous terms were applied to all kinds of uncleanliness whether moral or physical. In the Sanscrit Ayurvedas of Chacrata there is a full description of syphilis where it is regarded as constitutional, hereditary, and contagious. The poems of Martial, Juvenal, and Preapeia refer to it. Lunfranco of Milan, in the Middle Ages, separated the disease iuto three varieties. We must therefore date the origin of venereal far longer back than the end of the 15th century when some have^ presumed it first appeared.”
“On the other hand, there are numerous points of resemblance between syphilis and leprosy. Like secondary syphilis leprosy sometimes develops as an acute febrile eruption. Hoarseness and nasal voice, destruction of the palate and nasal bones, are common to both maladies. So are nervous affections. The tubercles of leprosy and the deposits of syphilis have so close a pathological resemblance that they cannot be satisfactorily differentiated, the resemblance of bacilli has been already referred to. Some writers have described a syphilitic leprosy, others have used the terms "leproid " or "syphiloid" for doubtful cases. But I think there is identity or at least as much identity as can exist between a parent disease, and its hereditary form. Whether we study what has been mentioned as a "superficial resemblance," or whether we study the "intimate pathology," it appears to me, that we find reason to conclude identity of the diseases.”

In a letter to The Lancet dated 1890, the author, A.D. Cooper, attempted to rebut an article published by Sir William Moore. In his rebuttal, Cooper noted the similarity between the diseases but felt that they should not trace pathological identities to “vivid resemblances.” Interestingly, he claimed that relying on an artificial classification system is only useful for clinical diagnosis but not for determining an etiological agent. Moore argued that acute febrile eruptions occur in both diseases, thus leading Cooper to question “why can we not say that all diseases which develop with acute febrile eruptions are identical?” Apparently, logic escaped him as this is precisely what should have been done but was instead ignored in an attempt to claim the same healing process was somehow distinct conditions. His further questions allude to the conclusion that should have been made had Cooper been intellectually honest with himself.
Does not syphilis mimic various non-specific forms of skin eruptions?
Are these diseases pathologically identical because there are "vivid resemblances"?
While Cooper admitted that syphilitic, lupus, and rodent ulcers on the face are very difficult to diagnose, he claimed that they “know” that there are different etiological agents for each, even though, at that point in time, the “etiological agent” for syphilis was not “discovered” for another 15 years. Cooper then admitted that the tubercles of leprosy and the deposits of syphilis are very similar in appearance, as well as lupus and tuberculosis. In fact, he stated that tuberculosis, together with the two, form the pathological group going by the name of "infective granulomata." He admitted that all three diseases were considered identical in the past. He also included both rickets and scrofula as also being considered as a part of syphilis. Cooper's rebuttal of Moore actually made a much better argument for why not only leprosy and syphilis are identical, but also tuberculosis, lupus, rickets, and scrofula as well:
ARE LEPROSY AND SYPHILIS IDENTICAL?
To the Editors of THE LANCET.
SIRS,-Sir W. Moore, in his able and learned article in THE LANCET of May 17th, endeavours to establish etiological identity between leprosy and syphilis. So far as I can judge, after a careful perusal of his article, I think that he has altogether failed in the attempt. He mainly relies upon the similarity of appearances for arguments in support of his theory. If we were to try to trace pathological identity in "vivid resemblances," we should be drifting into a hopeless condition of scientific embarrassment from which there could be no rescue. Is it necessary at this stage of medical science to remind Sir W. Moore that such attempts in the past have resulted in nothing but pathological chaos? It is at best an artificial system of classification and useful only for clinical purposes, being absolutely useless for throwing any light on etiological mystery. As such it has played an important part in the history of science, but now it had better remain a landmark in its evolution.
He says: Like syphilis, leprosy frequently develops as an acute febrile eruption develops." Therefore he argues that syphilis and leprosy must be identical diseases. The argument simply requires to be mentioned to carry its own refutation. Why can we not say that all diseases which develop with acute febrile eruptions are identical? He lays great stress on "vivid resemblances" between secondary eruptions of syphilis and leprous patches. I have spoken at some length on this point. I have pointed out the unscientific position in which we are placed by depending too much on "vivid resemblances." Polymorphism is the most characteristic feature of syphilitic eruptions. Papillary, vesicular, pustular, and various other intermediate forms, are found side by side indiscriminately in one and the same crop of eruptions. Does not syphilis mimic various non-specific forms of skin eruptions? Are these diseases pathologically identical because there are "vivid resemblances"? Are there not diseases etiologically identical and yet morphologically divergent one from the other as white is from black? Is not cancer hard and soft, now a fungating mass, then an extensive ulcer, and again a hard, firm cartilaginous nodule? There are diseases morphologically similar which are etiologically different. By morphological, I mean "in appearance." Syphilitic, lupus, and rodent ulcers on the face are very difficult to diagnose, but we know that they are all etiologically distinct one from the other. He says: "Hoarseness and nasal voice are symptoms of leprosy as of venereal." Do we ever find hoarseness and nasal voice as symptoms in any other malady which human flesh is heir to? I leave it to Sir W. Moore to answer this question. He goes on to observe: "Palate and nasal bones are sometimes destroyed in syphilis and leprosy." Have cancer and rodent ever played any mischief with the self-same bones? Is it rare to find leprosy attacking fingers and toes? Are these the favourite places of selection by syphilis? I grant that sometimes the tubercles of leprosy and the deposits of syphilis are very similar in appearance, but so is lupus, the tuberculosis of skin. Tuberculosis, together with the aforesaid two, forms the pathological group, which goes by the name of "infective granulomata." I should like to know if Sir W. Moore believes in the evolution theory of diseases. If so, he can assert a common parentage for all the three diseases, which, distinct today, were identical once. It is not for me to enter into a scientific speculation on etiology of diseases. For all practical purposes it is enough for me to know that tubercle, leprosy, and syphilis are distinct in their causation and in their natural history. Rickets and scrofula were considered as offsprings of syphilis, but regarded from the more modern point of view they are both independent of venereal. If Sir W. Moore wants to prove his theory to the medical profession, then it is incumbent upon him to prove that one merges imperceptibly into the other. He has not instanced one single case where a subject of inherited or acquired syphilis subsequently developed into a leper. I have never seen one such case, neither has any member of the whole medical profession of the world. Perhaps he has observed such cases. He must show us the reason why leprosy is practically unknown in this country, while syphilis, mild and severe, acquired and inherited, is as common as can be. We should like to know why syphilis (for all practical purposes) is amenable to treatment, while leprosy is not.
Sir W. Moore further remarks: "Improvement of treatment and improvement of sanitary surroundings, which include lodging, food, &c , may have eradicated one form of heredity." May I ask why not the other if etiologically the same? Cannot the same argument be, with greater force and plausibility, used by those who maintain that syphilis and leprosy were distinct in their origin and course. They may argue thus: it is precisely because both the diseases are distinct in their nature that one has disappeared while the other has remained unchecked. Environments, which are unfavourable to leprosy, do not seem to be unfavourable to syphilis. Has the withdrawal of the Contagious Diseases Act from Bombay in any way influenced leprosy as it has done syphilis? Perhaps the time is too short to pass any opinion. I am. Sir, yours faithfullv,
A. D. COOPER, L.R.C.P. Lond., M.R.C.S.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(02)19651-6/fulltext
At the end of his letter, Cooper challenged Moore to show “one single case where a subject of inherited or acquired syphilis subsequently developed into a leper.” Cooper claimed that he and all other members of the whole medical profession of the world had never seen such a case. I am not certain if Moore ever accepted the challenge. My guess is that he did not as the view of syphilis being a separate disease from leprosy persisted. However, less than a decade after the challenge was issued, such a case was observed. In a paper dated 1899, it was reported that a man was diagnosed with syphilis and underwent treatment. Upon doing so, he developed symptoms said to be leprosy. Instead of understanding that these symptoms are induced by the same healing process, they decided that the person was inflicted with both diseases at the same time. It was pondered if the treatment for syphilis, while “curing” the man of the disease, aggravated an underlying leprosy infection. However, this was considered unlikely and the case remained a mystery. Regardless, this case stands as an example where leprosy was said to develop after syphilis, thus meeting the challenge Cooper had set forth to Moore that he would have considered the required proof that these were, in fact, the same disease process:
SYPHILIS AND LEPROSY.
While the difference between leprosy and syphilis is now well established, the fact that they have in the past been confounded by some writers and the rarity of a coincidence of the two diseases in the same person makes the report of a case of primary specific infection in a leper of some interest. Such a case is recently reported by a Russian physician, Dr. Messaroche, in Wratch, and is noticed editorially in the Medical Press and Circular. The patient, a man, aged 47, presented himself "in the condylomatous stage of syphilis," but also had two small brown patches on the abdomen, and a hard swelling of the left testicle with edema of the scrotum of some standing. Under specific treatment the luetic manifestations disappeared, but a further crop of anesthetic brown patches on the abdomen made their appearance. The subsequent history of the case confirmed the diagnosis of leprosy, and its interest is in the fact that the disease appeared to be unaffected by the concurrent syphilis, unless we are to infer that an apparent aggravation under specific treatment was due to the disappearance of the latter. This was not apparently suggested or suspected by the reporter of the case, and may perhaps be considered as unlikely.
https://jamanetwork.com/journals/jama/article-abstract/475963
For a more recent case, a man was seen who had symptoms aligning with both syphilis and leprosy in 2019. The authors admit that the association between syphilis and leprosy is not well-documented. They decided to do laboratory testing for both conditions due to seeing matching clinical signs. Of course, the lab results pointed to both syphilis and leprosy and, thus, it was decided that this was a coinfection rather than the same healing process:
Syphilis and Leprosy Coinfection: A Challenging Diagnosis
“Background: The association between syphilis and leprosy is not well documented, and the emergence of isolated cases raises the interest and indicates that this dual coinfection can occur.”
“Key message: Few reports in the literature show coinfection of secondary syphilis and tuberculoid leprosy. In our patient, the simultaneous presence of syphilis and hansen’s diseases was demonstrated by the clinical history and laboratory investigation. We emphasize the importance of clinical suspicion for coinfection despite the polymorphism of these diseases as well as precise interpretation of laboratory and histopathology examinations to correctly manage atypical cases.”
Also in 2019, there was a case of syphilis that was said to mimic tuberculoid leprosy. However, the added caveat this time is that these conditions were seen in an HIV patient, thus we get a 3-for-1 scenario where three related conditions are seen in one patient. Clinical and laboratory findings made it necessary that leprosy was a part of the differential diagnosis. It was admitted by the authors that distinguishing between leprosy and syphilis is difficult and that these cases are seen in both HIV positive and negative patients. The tests used to definitively distinguish between the two are based on methods such as darkfield microscopy or PCR techniques, which are admitted to be only available to certain reference centers and have a relatively low sensitivity. Testing sensitivity refers to how accurate a test will be at detecting an etiological agent when it is actually present within a patient. Low sensitivity means that it fails most of the time:
Secondary syphilis mimicking tuberculoid leprosy in an HIV-positive individual: a case report
“Syphilis is a very polymorphous pathology in both its clinical and histological presentation. People living with human immunodeficiency virus (PLWH) are at increased risk for atypical or more aggressive presentations of secondary syphilis, including nodular or ulcerative lesions (lues maligna), keratoderma and enplaque lesions. Herein we present a case of secondary syphilis in person living with HIV with clinical and histological features suggesting tuberculoid leprosy. A high index of suspicion and complementary tests are mandatory for a correct diagnosis.”
“Histological examination in tuberculoid leprosy typically shows a dermal lymphohistiocytic granulomatous infiltrate following the course of a nerve. Acid-fast bacilli are usually not identified in paucibacillary forms. Since similar findings were noted in the present case along with a relevant clinical presentation, tuberculoid leprosy was part of the differential diagnosis.”
“It can be particularly difficult to distinguish between syphilis and leprosy. Previous syphilis challenging cases of syphilis have been described in both HIV-positive and HIV-negative patients. Definitive diagnosis of both entities is based on tests such as darkfield microscopy or PCR techniques, methods which are only available to certain reference centres and which have a relatively low sensitivity. In addition, both diseases are more prevalent in PLWH than in the general population.”
https://journals.sagepub.com/doi/abs/10.1177/0956462419869136?journalCode=stda
As a final example, this next case was a person diagnosed with leprosy, syphilis, and HIV. The authors admit that the skin lesions seen in HIV patients can resemble other diseases such as leprosy and syphilis and often lead to mistaken and delayed diagnosis. It is stated that coinfection between HIV, syphilis, and leprosy is rare and that it is not understood. The coinfection diagnosis was confirmed by the laboratory examinations which were acid fast bacilli for leprosy along with serological testing for syphilis and HIV. While claimed to be rare, how often are all three conditions tested for within a single patient? Perhaps this “rare” occurrence would not be so rare if clinicians regularly performed testing for each condition with every patient they see? Then again, with low sensitivity tests that fail most of the time, how would one ever be certain that the results were ever accurate to begin with? Interestingly, despite being diagnosed with three different conditions that typically require three different treatments, the treatment provided to the patient remained the same as if the diagnosis was separate.
Leprosy, Syphilis, and Human Immunodeficiency Virus Coinfection: A Case Report
“Clinical manifestasion of leprosy present with skin lesion from hypopigmented to nodular lesion and nerve damage (Ustianowski,2006). Likewise syphilis, the skin lesion can form ulceration, maculopapullar, to nodular (lynn,2004). Patients with HIV often have several simultaneous or sequential cutaneous conditions. In general, noninfectious cutaneous abnormalities are not prognostic of rapid progression of immunosuppression, but it might be specific markers of the stage of HIV disease (Maurer,1998). All of them can resembling other diseases and lead misstaken and delayed diagnosed for the clinician.
Coinfection between leprosy, syphilis and HIV are very rare, and their correlation remain unclear. This report is to present a man of 55 years of age diagnosed of leprosy with laten syphilis and HIV. Hopefully, this paper may remind clinicians the possible coincidence between these infectious diseases.”
“We reported a case of 55 years old man with BL/ LL leprosy, with latent syphilis, and HIV infection. The skin manifestation and histopathological were atypical, but these were supported by the laboratory examinations which were acid fast bacilli, serological test for syphilis and HIV serology. From this case, we demonstrate that coinfection between these three diseases is apparently possible, make the clinical and histological features may be atypical, as interactions each other between them. In general, the therapy is the same as the disease was separately.”
Syphilis and HIV
The difference between syphilis and HIV infection is complex and remains incompletely understood, despite there being more than 2-decades of clinical experience with co-infected patients.
https://www.bestonlinemd.com/difference-between-syphilis-and-hiv/
This brings us to the next connection that is rarely investigated, that regarding the similarities between syphilis and AIDS. Both of these conditions are claimed to be sexually transmitted. They present with similar signs and symptoms and have latent periods without symptoms of disease that can last for decades, if not indefinitely. Numerous other unrelated conditions are contained within their umbrella of associated diseases. The toxic treatments (mercury/arsenic/penicillin for syphilis and AZT/ARV's for HIV/AIDS) that are used to combat the conditions are more deadly than the diseases themselves. The symptoms caused by these poisons became incorporated into the disease description. For all intents and purposes, syphilis and AIDS are the exact same monster that was fraudulently labelled with different names. Besides the name change, the only difference between the two is the unproven etiological agents whereas one is a bacterium and the other is a “virus.”
When exploring this connection, the first thing to note is that, when HIV/AIDS appeared and cases began increasing in the 1980's and 1990's, syphilis cases began to plummet. This is always a dead giveaway that the same symptoms of disease have been relabeled and are being given a preferential diagnosis with the hot new name and cause. According to data by the CDC, while syphilis cases increased prior to AIDS, as the AIDS epidemic became more prominent in 1983, the national cases of syphilis began to drop. They claimed that the media attention on AIDS may have indirectly affected the rates:
Syphilis -- United States, 1983
“Although the incidence of primary and secondary syphilis in the United States steadily increased from a low of 9.4 cases per 100,000 population in 1977 to 14.6/100,000 in 1982, the reported national incidence decreased to 14.1/100,000 in 1983 (Figure 1). Reported primary and secondary syphilis cases totaled 32,698 in 1983, a 3% decrease from the 33,613 cases reported in 1982.”
“The decrease in the national incidence of reported syphilis cases may represent, in part, a response to public health recommendations to decrease risks of sexually transmitted diseases (2). With the media attention given acquired immunodeficiency syndrome (AIDS) and herpes, syphilis rates may be affected indirectly, as gonorrhea rates have been in certain localities (3,4).”
https://www.cdc.gov/mmwr/preview/mmwrhtml/00000381.htm
In England, a similar trend was witnessed in that there was a massive decline in nearly all non-HIV STD's. Syphilis went from 1500 cases annually in the mid-1980’s to 150 cases by the mid-1990’s, while HIV cases were stabilized and began increasing in the late 1990’s:
The 1980s AIDS campaign
“Although the target of the campaign was HIV, it actually had a profound effect on all sexually transmitted infections. Following the campaign, the number of diagnoses of gonorrhoea in England and Wales dropped from around 50,000 in 1985 to just 18,000 in 1988 - and had dropped to a 20th century low by the mid 1990s. Syphilis dropped from around 1500 annual cases in the mid 1980s to around 150 in the mid 1990s.”
New diagnoses of HIV, which were over 3,000 in 1985, dropped by a third in three years. The number of new diagnoses stayed relatively stable until 1999. It has since more than doubled to 7,000 new diagnoses each year.”
http://news.bbc.co.uk/1/hi/programmes/panorama/4348096.stm
Another indicator is what happens between the cases of each disease when a new treatment comes around, such as with the introduction of the slightly-less-toxic-than-AZT antiretrovirals (ARV's) in the late 90's to treat HIV. As HIV/AIDS cases fell in the late 90's and early 2000's in order to create the appearance that the ARV treatments were effective, syphilis cases began to rise once again. Thus, there is a clear relationship between these diseases whereas when the cases of one increases, the other decreases, and vice versa:
An Update on the Global Epidemiology of Syphilis
“In the late 1990s, the prevalence of syphilis plummeted in many countries with endemic syphilis, largely thought to be due to the introduction of syndromic management for STIs [50, 51], behavioral changes, and the effect of AIDS mortality disrupting sexual networks [52-54]. However, since the introduction of antiretroviral therapy (ART), rates of syphilis have increased, especially among MSM, perhaps due to the reconstruction of sexual networks and increased frequency of sexual contact [55, 56].”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6089383/?report=reader

Highlights from this next source show some very interesting links between syphilis and HIV/AIDS. The article starts by focusing on the stigma that was placed upon those who were labelled with syphilis and were ultimately treated with the toxic mercury “cure.” The disease was considered divine retribution for the “sexual union between man and monkey,” which draws parallels with HIV today. The majority of the cases of syphilis are reported in people who are HIV positive. As the sores resemble each other so closely, it is said that a syphilis diagnosis may be harder to detect in HIV patients. In studies conducted before the use of ARV's, it was concluded that having syphilis may be a cofactor that sped up the progression from HIV to AIDS. Thus, it is clear that these conditions are inextricably linked.
What is very interesting about this article is that it presents two cases showing the syphilis/HIV connection. The first is of a man named Kelly who tested for syphilis after getting a divorce and finding multiple sexual partners in a local bathhouse. His blood tests showed latent syphilis (i.e. no symptoms), so his doctor recommended a spinal tap to make sure there was no neurological involvement, which came back negative. He received the standard 3 injection penicillin treatment in order to “cure” his infection. Due to his syphilis status, he was tested for HIV which ultimately came back positive as well. This situation is similar to what had happened to my relative, granted there were no sexual partners involved and the testing and treatment were essentially forced. The penicillin injections used as a “cure” are toxic and can lead to a rapid deterioration in a person's health. The HIV diagnosis came after the syphilis “cure.”
The second case presented was of a woman named Sheila. She had noticed a sore on her leg and thought that it was nothing but a bite of some kind. After the urging of a friend, she tested for syphilis and HIV. Both came back positive. Sheila is now a public speaker who includes syphilis in the discussion in her AIDS talks as she felt that there was not enough awareness about the connection between the two diseases.
The article goes on to mention that some view syphilis as a cofactor that leads to AIDS and that there is a synergy between the cases. If there are spikes in syphilis, they claim that there are spikes in AIDS as well. It is stated within the article by Sandra Larsen, MD, a syphilis specialist for the CDC, that syphilis can “mimic” the same opportunistic infections and cancers as well as the same symptoms of AIDS. Thus, they started testing AIDS patients for syphilis who had symptoms associated with tertiary syphilis even though these people had tested negative for syphilis in the past. It was claimed that these cases were “missed” somehow. Repeated studies had shown that syphilis infection and, particularly, reinfection, was not being detected with current tests. The CDC had estimated that there were 325,000 cases of untreated syphilis at the end of the 1970s that somehow disappeared. Thus, they are now working on ways to utilize PCR, serological, and antigen tests to try and pick up these ‘missed” cases of syphilis that mysteriously vanished with the rise of AIDS:
The Secret Life of Syphilis
“Syphilis, for centuries so feared that it was known as the “great” (as opposed to the small) pox, has been distinguished as much by the desire to blame it on others as for its power to destroy. Medieval cities banished syphilitics outside their gates or “cured” them with mercury ointments that made their bodies shake and teeth fall out before they died. In the U.S., well into the 20th century, syphilitics were subject to toxic treatments both physical and moral: expensive, ineffective drugs as well as public condemnation as “plague spots” and infectors of “innocent victims.” Those theorizing the origins of syphilis have pointed to distant continents and unspeakable acts: Columbus’ voyage to America, government conspiracy (Spaniards, it was said, mixed lepers’ blood with Greek wine), or those perennial favorites -- divine retribution and sexual unions between man and monkey. Ring a bell?
Today, post-penicillin and in comparison with AIDS, the great pox seems more like small potatoes. Yet for those wrestling with HIV, Treponema pallidum -- the corkscrew-shaped bacterium (spirochete) that causes syphilis -- is both past lesson and present danger. Over the past two years, outbreaks have been reported in many urban centers; in virtually all of them, the majority of cases have been among people with HIV. Syphilis -- or, more accurately, the sores (called chancres) or rashes it causes in its early stages -- heightens risk of HIV transmission and may be harder to detect in HIVers. Doctors have reported cases of syphilis progressing to its fourth, most neurologically damaging phase (see “The Four Seasons of Syphilis” below) in a matter of months, as opposed to years, among people with weakened immune systems. And some pre-HAART era studies have found that having syphilis may be a cofactor that speeds progression from HIV to AIDS.”
“Kelly, now 45, got a health department call at his job in Salt Lake City, Utah. Recently divorced and still closeted, he had been finding sex partners in the only place he felt safe looking -- the local bathhouse. This was early in the AIDS epidemic, and the health department’s call was the first sign he’d had that playing with men was “real life, not just pure fun.” His blood tests (see “Sussing Out Syphilis” below) showed latent syphilis, so his doctor recommended a spinal tap to make sure there was no neurological involvement.
The test showed no spinal fluid abnormalities, so Kelly got rid of his infection with standard treatment for latent syphilis: injections of penicillin, “once a week for three weeks in alternate buttocks.” But his syphilitic status, however temporary, was a clue to a more enduring health challenge. “If it wasn’t for the syphilis, I wouldn’t have thought about taking an HIV test,” Kelly says. “As it was, I waited a while. Later, my new boyfriend and I both went in. I was positive. So was he.”
“Sheila, 32, is a Wake County resident who understands firsthand the value of outreach. “I never heard anything about syphilis until I was going to get treated,” she says. "I had a sore on my leg -- I’d thought I’d gotten bit by something. A friend said, ’Girl, don’t you know what that is?’“ Sheila’s positive syphilis test led her to work up the resolve for an HIV test -- also positive. Nine hospitalizations later, she’s feeling well and volunteering for a Raleigh AIDS organization, where she folds syphilis into her AIDS talks. ”Even with all this emphasis on HIV, you don’t hear much about other STDs,“ she says. ”I honestly believe that if there had been people out there talking about how to protect yourself, I would have been safer."
Silence around syphilis, say some researchers, may extend from the streets to the research lab. Despite widespread skepticism, they see in syphilis a cofactor or even a cause of AIDS (see "The Case of the Missing Cofactors," POZ, April 2000). They point not only to the epidemiological synergy between syphilis and AIDS -- spikes in syphilis regularly precede new AIDS epidemics worldwide -- but to the medical literature before the age of antibiotics. “TB, rare cancers and pneumonias -- all of these were documented, if unusual, expressions of syphilis before the antibiotic era,” says Joan McKenna, a research physiologist whose 1986 article in the journal Medical Hypotheses first presented the AIDS-syphilis connection.
McKenna found an unlikely ally in Sandra Larsen, MD, then a syphilis expert at the CDC. “The clinical manifestations of syphilis, which have taken various forms over the century, have now been transformed to mimic the appearance of the opportunistic infections and cancers that may accompany HIV infection, as well as the clinical symptoms of AIDS itself,” Larsen wrote. McKenna began sending AIDS patients in for confirmatory syphilis tests, even when they’d first tested negative. “We had people showing up negative on the initial tests even when they had known infections and tertiary symptoms,” she says. “These syphilis cases were being missed.”
McKenna is now a minister at the Vaca Valley Church of Science in Fairfield, California (“the same church as Louise Hay,” she notes), and Larsen is retired from the field. Others interested in the AIDS-syphilis link scrapped the theory in the late ’80s, when doctors treating HIVers with IV antibiotics found that they still sickened and died. But the idea that a new form of chronic syphilis may be mistaken for HIV-related infections, has been kept alive by Toronto researcher John Scythes and colleague Colman Jones. “Repeated studies show that syphilis infection and, particularly, reinfection, may not be detected with current tests,” Jones says. “So some of those we say are cured of syphilis may instead be being missed. The CDC estimated there were 325,000 cases of untreated syphilis at the end of the 1970s. Where did they go?”
“Eventually researchers may be able to culture the syphilis spirochete from long-infected patients in the same way they cultured the Lyme spirochete. In the meantime, a number of companies are developing assays capable of picking up syphilis that existing tests miss. “There are many such tests in development,” says Robert Baughn, PhD, of the Department of Microbiology at Baylor College of Medicine in Houston, Texas: "There’s a western blot test, PCR tests that extract genetic material from the spirochete, as well as a number of tests using recombinant T. pallidum antigens rather than antigens used by the standard confirmatory tests." None has yet been approved for clinical use, though at least one recombinant antigen test, called TrepCheck, has shown greater sensitivity than standard assays in prelimary research.”
https://www.poz.com/article/secret-life-syphilis
This next source discusses how a surge in syphilis cases mimicked HIV, right down to targeting gay men, injection-drug users, and those having sex for money and drugs. It is said that, early on in the HIV epidemic, coinfection with syphilis made the syphilis symptoms worse, which is a reversal of the previous source stating syphilis sped up the transition to AIDS. The HIV positive patients with syphilis may have multiple chancres compared to their negative counterparts. They may experience the symptoms of both primary and secondary syphilis at the same time. These patients may progress to tertiary syphilis faster than others. They may also experience optic neuritis, uveitis, and other ocular manifestations of syphilis more commonly. What is unfortunately missing from this article is that it is well-known that ARV's can cause many of these worsening symptoms which are seen in HIV patients. Thus, it is no mystery why those who are HIV positive may experience worse symptoms than those who are negative. HIV positive patients are commonly subjected to longer and more toxic treatments than their negative counterparts.
The article goes on to explain that testing for syphilis in HIV patients can be tricky for a variety of reasons. There can be unusual and contradictory antibody results, false-negative and/or delayed positives, and false-positive results due to cross-reactivity. In other words, the test results are highly unreliable, and they have an excuse ready for every occasion. Due to thus unreliability, clinicians are advised to treat HIV patients as positive for syphilis if it is suspected and to overtreat them to err on the side of caution:
Syphilis and HIV: The Intersection of Two Epidemics
“Similar to the HIV epidemic, the current syphilis epidemic predominantly affects three groups: men who have sex with men (MSM), injection-drug users, and individuals who engage in sex for money or drugs. The CDC estimates that, in 2008, MSM accounted for more than 60% of all new diagnoses of primary and secondary syphilis in the U.S.7 Women account for a much smaller proportion of cases, but the incidence in this group has been increasing during the past 10 years7 — a trend that could be related to the high proportion of MSM who engage in sex with women. In one study from sub-Saharan Africa, that proportion was >90%.8”
“Whether HIV infection alters the natural history of syphilis remains controversial. Early in the HIV epidemic, case reports and case series suggested that HIV coinfection results in a more aggressive course of syphilis.12,13,14 However, more-recent studies describe only a few notable differences in presentation, which likely occur as a result of immune dysfunction among HIV-infected patients.15,16,17 Those differences are highlighted below, with more detail in Table 1. opens in new tab:
HIV-infected patients may present with multiple chancres that are deeper and slower to resolve than the solitary chancre typically seen in HIV-uninfected patients.1,18
Primary and secondary syphilis overlap more often in patients with HIV infection than in those without.13,15 In fact, one quarter of coinfected patients present with concurrent primary and secondary disease.1
HIV-infected patients may progress to tertiary syphilis more rapidly than HIV-uninfected patients, resulting in earlier onset of cardiovascular and neurologic sequelae.19,20,21,22
Optic neuritis, uveitis, and other ocular manifestations of syphilis are common among HIV-infected patients but not among HIV-uninfected patients. This atypical presentation of syphilis is clinically important: One study showed that 85% of HIV-infected patients with ocular syphilis had concomitant neurosyphilis.23
Given these differences, clinicians should have a heightened suspicion for neurosyphilis among HIV-infected patients, particularly those presenting with ocular symptoms.”
“In most instances, serologic testing for syphilis is reliable in HIV-infected patients, especially those who are not significantly immunocompromised. However, problems may arise in the following scenarios:
Unusual serologic responses, such as higher-than-expected titers. In one study, the geometric-mean RPR titer was generally higher among HIV-infected than HIV-uninfected individuals, particularly during secondary syphilis.16 Inappropriate B-cell activation as a result of concomitant HIV infection may be responsible for this finding.
False-negative results or delayed seroreactivity. False-negative results may be due to either prozone phenomena (nonvisualization of agglutination as a result of an overabundance of antibodies interfering with clumping of antigen-antibody complexes) or B-cell failure in late-stage HIV infection.26 Impaired responses to polysaccharide and protein antigens have been reported among HIV-infected individuals, making serologic diagnosis of some infections, including syphilis, unreliable.27 In fact, at least two cases of seronegative secondary syphilis have been reported in patients with AIDS.28,29
Biological false-positive results, as a consequence of HIV infection and antigen cross-reactivity. Such false-positive results can occur, but clinicians must be careful not to attribute positive nontreponemal test results to HIV infection alone, even when the titers are very low. This could lead to undertreatment of syphilis in a high-risk population, which would have serious downstream public health consequences.
When serologic results seem questionable, clinical and laboratory data should be considered together in arriving at a proper diagnosis. If uncertainty remains, it is probably best to err on the side of overtreating to avoid potential long-term clinical and public health consequences.”
https://www.jwatch.org/ac201009030000001/2010/09/03/syphilis-and-hiv-intersection-two-epidemics
The above information about the tests was confirmed in this next source which stated that testing for syphilis is unreliable and cross-reacts with HIV antibody tests. However, even if syphilis is suspected, it is difficult to diagnose due to its uncanny ability to mimic so many diseases and a definitive listing of the signs and symptoms can not be produced for a differential diagnosis. It is said that tests can be modified and/or take longer due to syphilis infection with HIV. Testing is also unreliable when examining lesions in the mouth as it is claimed that there are non-pathogenic treponemes that are identical and can be confused with T. pallidum. Because of this unreliability, other tests are used to make a diagnosis which are considered unreliable as well. The first is an antibody test called reagin which can test positive for many other conditions other than syphilis, thus it cannot be used for diagnosis. The T. pallidum particle assay test, enzyme immunoassays and tests for “specific” IgM are also utilized to try and get an accurate diagnosis. However, it is admitted that these tests are difficult to interpret and that they cannot distinguish between infection caused by T. pallidum and those caused by other treponemes. In other words, they are worthless as well. As the tests can not accurately diagnose syphilis and the HIV test cross-reacts with the biological markers associated with syphilis, there is no way to say that HIV/AIDS cases are not, in fact, syphilis cases:
Syphilis and HIV infection
“The clinical course of, and serological tests for syphilis can be modified by concomitant HIV infection. Of notable importance, serological tests can take longer to become positive, while the development of neurosyphilis can occur more rapidly compared with the situation in patients who are not infected with HIV.
Laboratory diagnosis of syphilis
Since infection with syphilis can mimic numerous medical conditions it is difficult to construct a useful list of all the signs and symptoms for which a diagnosis should be considered. As the eminent physician Sir William Osler once said: ‘he who knows syphilis knows medicine’. As a generalisation, all patients presenting with neurological symptoms should be tested for syphilis, as should pregnant women and patients with other venereal diseases.
Facilities for carrying out dark-ground microscopy to look for treponemes are available in few laboratories. Furthermore, this test is unreliable when examining lesions in the mouth as non-pathogenic treponemes can be confused with T. pallidum. However, there are two groups of tests that can be used:
Reagin tests detect antibodies to cardiolipin, though they can be positive in conditions other than syphilis. Though they are not diagnostic for syphilis, they are helpful for monitoring the response of a patient to treatment once diagnosis has been confirmed by a specific test. The Venereal Diseases Research Laboratory (VDRL) test is a reagin test.
Specific tests include the T. pallidum particle assay test, enzyme immunoassays and tests for specific IgM.
The results of serological tests can be difficult to interpret, so guidance should always be sought from a consultant microbiologist or a consultant in genitourinary medicine. Any patient with positive serological tests for syphilis should be referred to a consultant in genitourinary medicine.
Serological tests for syphilis cannot distinguish between infection caused by T. pallidum and that caused by other treponemes, such as the causative agents of yaws and pinta.”
https://wchh.onlinelibrary.wiley.com/doi/10.1002/tre.788
The Great Imitators
Beyond the failure to accurately distinguish between syphilis and HIV in the laboratory, there is another similarity between these two diseases. Just as syphilis became known as “the great imitator” throughout its vast history, so too, did AIDS. In fact, it became the “new great imitator” signifying its replacement over the previous disease bearing the moniker, especially as it absorbed into its own umbrella the neurological symptoms associated with syphilis:
AIDS: The New “Great Imitator”
“The first edition of Russell Brain's Diseases of the Nervous System (1933) states that “Syphilis is the most frequent disease of the nervous system and is the cause of one in every seven cases of organic nervous disease.” ‘New observations concerning acquired immune deficiency syndrome (AIDS) evoke these grim historical perspectives regarding the actual and potential similarities between AIDS and syphilis. Acquired immune deficiency syndrome has now also become a “great imitator’” certainly insofar as the neurological syndromes which are being delineated. These neurologic syndromes, especially AIDS dementia, are increasingly noted in patients with no other clinical manifestations of AIDS or AIDS related complex (ARC).2–5”
https://agsjournals.onlinelibrary.wiley.com/doi/full/10.1111/j.1532-5415.1987.tb04672.x
However, AIDS is not the only other disease to earn that distinction of being referred to as “the great imitator” along with syphilis. It wasn't even the first. Prior to the 1987 declaration, in 1961 it was tuberculosis, another condition said to be regularly confused with both syphilis and HIV, that was also given this title:
The Second "Great Imitator"—Tuberculosis
“IT HAS LONG BEEN KNOWN that syphilis is capable of mimicking many other diseases. That tuberculosis can also imitate various other conditions is less emphasized. However, an awareness of the atypical clinical manifestations of tuberculosis is increasingly important since the index of suspicion of a disease tends to subside with its decreasing prevalence.”
https://jamanetwork.com/journals/jama/article-abstract/331211
Another condition often confused in the diagnosis of both syphilis and HIV is lupus, an autoimmune disorder that can occur in stages and presents with the same symptoms such as rashes, sores, fever, weight loss, and the ability to damage the nervous system. It is said that lupus also affects the HIV laboratory results and can trigger “false-positive” HIV diagnoses as well. As with the diseases listed before, lupus also earned the name “the great imitator” due to its varying presentation:
Lupus: The Great Imitator
“Lupus is a tricky disease, masquerading as a variety of conditions. This results in an average of six years between the onset of symptoms and the time a person receives a diagnosis. We’re breaking down the basics of this mysterious condition so you can better track your symptoms.”
“People call lupus “the great imitator” because its symptoms often mimic those of other conditions, including fibromyalgia, diabetes, and Lyme disease. A person with lupus might experience changing symptoms, and the signs can come and go or vary in severity over time, making the condition difficult to diagnose.”
https://www.stlukeshealth.org/resources/lupus-great-imitator
Lyme disease is yet another condition often confused with syphilis and HIV. It can also come in stages, and it is said to cause multisystem disease particularly affecting the skin, nervous system, heart and musculoskeletal system. Like T. pallidum, the Lyme disease bacterium Borrelia burgdorferi is a closely related spirochete, i.e. they look identical. Probably unsurprising at this point, Lyme disease is also a “great imitator” as well:
Lyme disease: the latest great imitator
“Lyme disease is caused by the spirochete B. burgdorferi. Like its counterpart syphilis, it causes multisystem disease particularly affecting the skin, nervous system, heart and musculoskeletal system. It is endemic in several areas of the United States as well as in Europe. The prompt recognition of this disease and its diverse manifestations should lead to early treatment and resolution. Prevention is aimed at avoidance of the tick vector.”
https://pubmed.ncbi.nlm.nih.gov/3292999/
And finally, we come full circle back to leprosy, which has also been given the distinguished honor of being known as “the great imitator.” While leprosy may be the forgotten condition in favor of syphilis, AIDS, lupus, Lyme, and tuberculosis, it still exists today and can cause great difficulty for clinicians trying to get an accurate diagnosis. It is said to have a wide range of clinical presentations and that it is because of this diagnostic dilemma that it has earned the title with other “great imitators:”
Leprosy: A great imitator
“In recent years, advances in medical diagnosis and treatment have greatly attracted our attention, whereas some rare diseases, such as leprosy, have not found a place in the medical education curriculum; their existence may even be forgotten. Although the prevalence and incidence rates for leprosy have been significantly reduced as a result of the control strategies of the World Health Organization, new cases still appear. A total of 214,783 new cases were reported from 143 countries during 2016, corresponding to the global new-case detection rate of 2.9 per 100,000 population. Leprosy proves to be a very interesting model due to its immunologic properties. It joins with syphilis, mycosis fungoides, cutaneous tuberculosis, and sarcoidosis as one of the great imitators. The diagnosis of leprosy can be simple and practical, but considering the diagnosis of leprosy in the differential diagnosis is the first requisite again.”
“Leprosy is a mutilating and stigmatizing disease with a low rate of infectivity and a wide range of clinical presentations. It causes a great diagnostic dilemma, justifying the description “the great imitator.” In endemic areas, it is imperative to keep in mind the “many faces of leprosy” to prevent misdiagnosis. There is still a need for developing new and better diagnostic tools and treatment methods to achieve early diagnosis and treatment of leprosy and its complications.”
https://www.sciencedirect.com/science/article/abs/pii/S0738081X19300021?via%3Dihub
As can be seen, history is full of great imitators when it comes to so-called pathogenic diseases. These diseases are all connected as they are all signs of a healing process that has been fraudulently broken into separate conditions. However, from leprosy to syphilis to AIDS, there are no specific symptoms that belong to only one disease. These conditions all overlap and can be associated with the same signs and symptoms of each other. The only slight difference is in the theoretical models that are built into some regarding different stages as well as the fictional etiological agent they are linked with, whether bacteria, “virus,” or something presently unknown. These diseases can not be diagnosed based on clinical symptomology alone due to the many shared similarities. Thus, the only way to distinguish between the conditions is based upon inaccurate molecular tests that are entirely unreliable. When the lab results come back for multiple conditions, this contradiction is simply explained away with the excuse of coinfections. This ability to blame the same symptoms on different etiological agents covers up the conflicting test results and the inability to diagnosis clinically. It conveniently provides the “viral” pseudoscience with its cloak of un-falsifiability.



{kind=link}
I think Lanka once said something about The Vatican setting some proto medical council to ascertain or determine leprosy - with a local official and a Papal representative.
the result of a 'negative test being banishment or social exclusion which usually meant a death sentence. Whatever intension may have set it up, it became a political tool.
Id like more info around that - but the pattern is recognisable.
From a bio of Captain Cook (v good!) posited the open sexuality of Polynesians or Tahiti (eventually resulted in VD attributed to the sailors.
German New Medicine's biological conflict expressing as poxes is often around a self-dirtying or feeling soiled conflict. Such conflicts can loop (ie reset themselves as persistent) or reappear from associative triggers.
We might assume mind and world the same but people believed silly things in the past, but I suggest our experience of self and world have radically changed. But as can be readily observed the underlying traumas and survival strategies run back to when Mars acquired the name 'Scarface' and a poxed face - as perhaps did many as a result of nanoparticulate poisons from volcanic actions and cosmic dust - both associated with electromagnetic disturbances - and famine from blocking the Sun Malnutrition).
I don't offer psychic aspects to 'explain' but to complement our experience.
The wish for a diagnosis would be to escape the fear of stigma. That this may still occur is at least counters by the attribution to microbes etc BUT insofar as we set the cause of our experience exclusively out and away from self, we set ourselves victim to them & THEIR TREATMENTS!
Wholeness of being as a felt quality of life and vitality is lost to self-conflict, or in some sense hostage to rules and filters of permission to live our freedom.
I've been looking at zeta-potential as an underlying biophysical basis of blood sludge, micro-strokes (TIAs). amidwesterndoctor gives a good background and outline - Andrew Moulden was the first to alert the clinical signs. But if you are not aware of this angle - please look.
https://amidwesterndoctor.substack.com/p/what-actually-happens-with-water
Zeta potential article
https://amidwesterndoctor.substack.com/p/why-does-every-vaccine-often-cause
He doesn't GET the basis for calling out virus fraud. But I am glad to not let that stop me reading his contributions.
'Stress proteins' were noted in a study :
DNA is a fractal antenna in electromagnetic fields
* April 2011
* International Journal of Radiation Biology 87(4):409-15
DOI:10.3109/09553002.2011.538130
* Source
* PubMed
Authors:
Martin Blank
* Columbia University
The realm of bio-field is cutting edge bio-hack.
At least as the attempt intent to marketise or weaponise (another gold rush for investors to then drive the narratives that become too big to fail - as with genes and germs/virology).
Abstract
To review the responses of deoxyribonucleic acid (DNA) to electromagnetic fields (EMF) in different frequency ranges, and characterise the properties of DNA as an antenna. We examined published reports of increased stress protein levels and DNA strand breaks due to EMF interactions, both of which are indicative of DNA damage. We also considered antenna properties such as electronic conduction within DNA and its compact structure in the nucleus. EMF interactions with DNA are similar over a range of non-ionising frequencies, i.e., extremely low frequency (ELF) and radio frequency (RF) ranges. There are similar effects in the ionising range, but the reactions are more complex. The wide frequency range of interaction with EMF is the functional characteristic of a fractal antenna, and DNA appears to possess the two structural characteristics of fractal antennas, electronic conduction and self symmetry. These properties contribute to greater reactivity of DNA with EMF in the environment, and the DNA damage could account for increases in cancer epidemiology, as well as variations in the rate of chemical evolution in early geologic history.
I don't share the storied assumptions of the article BTW - but I note of DNA biofield interactions that I associate with structured water (at nano-scale not just EZ) UPSTREAM to the gene doma of a physical (closed system) determinism. Proteins 'do their thing' in and by structuring/destructuring or phase changes that fold/unfold synthesise/replicate as translation of field information to mediums of differing response.
That might account for proteins that can be triggered by application of fields or modification of the medium and then assigned to 'transfection' (which is the man made version of what a virus is asserted to do.
It remains possible emf (not just 5g or even man made emf) contributes to a weakening of zeta potential (vitality and resilience of the living organism) - possibly by blocking communications for healing rebalancing - for the Biofield of Earth/Cosmos is our living context - not a separate thing.
And it remains possible that stealth exposures generate what is defined as 'spike protein' such as lipid nanoparticles - but even so these are colloidal or clumpy according to zeta potential - so even if NOT 'weaponised' or coordinated to act in synergy - they do.
If we WANT a good story that truth can wait on our experience to tire of - then we find or make one. That is 'gaming addiction' to effectively run on and as 'game theory' which is another level of modelling that is being applied to our world via predictive modelling instead of living relationships - (that are being replaced by zero-trust as zero tolerance for risk).
The idea that our consciousness is the primary effect or alignment of our own field but that we can assign responsibility externally and so suffer as if at the hand of an other has to then realise we use our mind to depreciate our mind. Like the idea of using 100% of our mind to give ourselves the experience of using only 1% or is that 0.001%? (Progressive limitation as a result of an out-of-control, control mentality).
None of our models is more than a set of definitions by which to generate experience - that may be more or less resonant/disonnant with felt nature (not our defined 'nature').