I was recently in a discussion on Twitter with a user who was utterly convinced in the power of vaccination to end “viral” diseases. This person believed that smallpox had been successfully wiped off the face of the Earth through the injection of toxins directly into the bloodstream and that the defeat of polio was well within our grasp through these same methods. It did not matter one iota to this individual that the evidence supporting the belief that vaccines led to a decrease, and in some cases “elimination,” of a particular disease was entirely fraudulent. No matter how hard I tried to pull the curtain back in order to reveal the magic tricks that had successfully led to the diehard indoctrination, this person resisted and fought feverishly to maintain the illusion. The cognitive dissonance was unfortunately too strong to overcome.
While I may not have reached this one individual, I never let a good opportunity to help others pass me by. Throughout the conversation, I was reminded of previous research I had done regarding the sleight of hand used with the polio and smallpox vaccines to make them look successful. While the official narrative was that the vaccines prevented the transmission of the invisible “viruses” which stamped out the associated diseases, there were more obvious reasons for the apparent decrease in cases. As I felt that I had just barely scratched the surface of this subject previously, I felt compelled to dig a bit deeper during this conversation in order to present the information as faithfully and as accurately as possible. I am collecting that information here in the hopes that this article can be used in the future to help break the indoctrinated free from this vaccine spell that they currently find themselves a slave to.
"The decline in infectious diseases in developed countries had nothing to do with vaccinations, but with the decline in poverty and hunger." - Dr Buchwald, M.D.
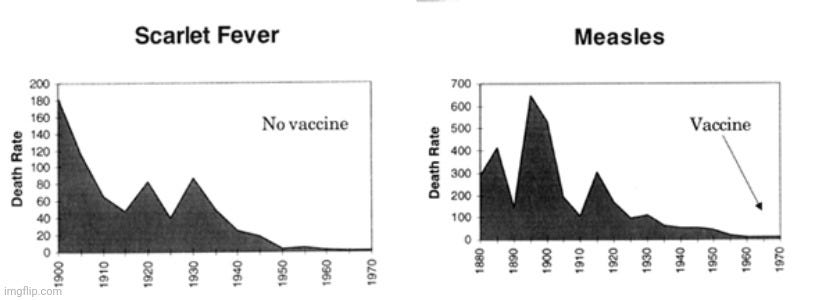
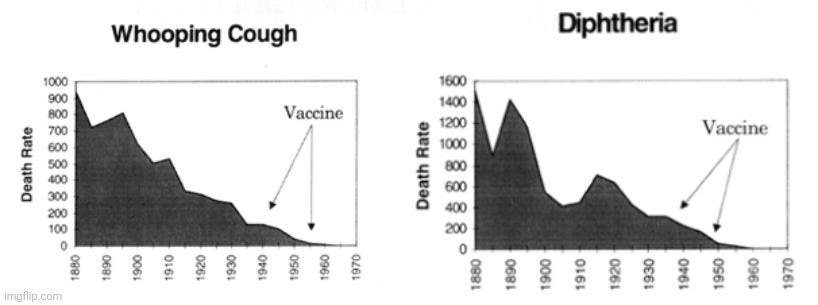
While we have been regularly subjected to the praises of vaccination with stories promoting the magical abilities of these unnatural injections to stop disease, when one looks at the statistical evidence collected over the years, an entirely different picture emerges. For instance, the below charts were taken from Greg Beattie's book "Vaccination A Parent's Dilemma." The graphs were created from the official death numbers recorded in the Official Year Books of the Commonwealth of Australia.
It is clear that many of the diseases that are commonly vaccinated for decreased dramatically before any vaccine was ever introduced. In fact, both Typhoid and Scarlett fever declined without any vaccine whatsoever. These same trends were noted in other countries such as the USA and England. The improvement in these diseases was not due to vaccines but were instead the direct result of better sanitation and waste removal as well as easier access to fresh food and clean water. There is no reason to give any vaccine credit for the sharp drops in disease already in a steep decline prior to their introduction. For more on these precipitous declines, please see this excellent article on Whale.to.
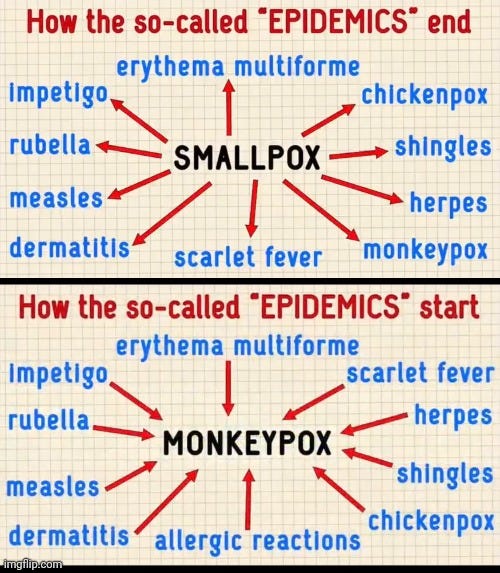
The realization that these diseases declined without the presence of any vaccines is pretty damning in and of itself. However, there is a trick that is regularly utilized in order to create the illusion that the introduction of a vaccine was the reason for any decrease and eventual disappearance of a specific disease and its associated “virus.” This trick is the reclassification and rebranding of the exact same symptoms of disease into many other separate and new diseases. This shuffling of the same symptoms into different categories is another factor, along with better sanitation and nutrition, for a perceived decrease in these diseases. This can be easily demonstrated by looking at both smallpox and polio as, even though these diseases are said to be either “eradicated” or close to it, the same symptoms still persist under various other names. Let's take a look at both of these situations and see what we can reveal about the magician's tricks.
Smallpox Reclassified
Taken from the excellent Kate Sugak presentation linked below.
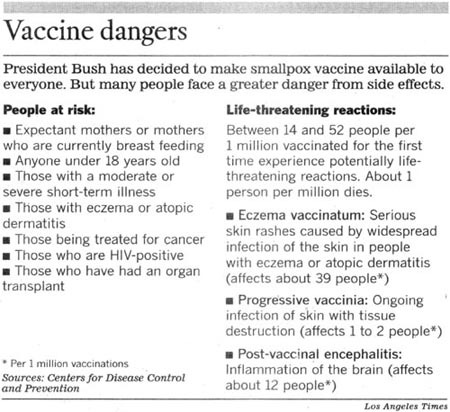
While a smallpox vaccine had been available since the late 1700's, this pesky disease, said to be caused by the “variola virus,” still hung around for nearly two more centuries. By the mid-20th century, smallpox was claimed to be eradicated from America and other industrialized nations even without mass vaccination campaigns. However, third world countries were still being ravaged by this disease. Thus in 1958, the WHO called for a global eradication effort utilizing what has been referred to as “the most dangerous vaccine known to man” to finally stamp out this disease once and for all. Interestingly, that same year, the identical in every way “monkeypox virus” was “discovered” in cynomolgus monkeys. What an amazing coincidence, right? This new “virus” eventually made the leap into humans a decade later when an infant came down with smallpox in Zaire. However, the child's village had been declared smallpox free due to the mass vaccination of the entire village the year before. If smallpox was allowed to be diagnosed in a “smallpox-free” zone, this could have easily led to questions regarding the vaccine’s effectiveness. Thus, after initial testing diagnosed the child with smallpox, further testing was carried out by the CDC. It was ultimately decided that this child was not a smallpox case but was instead the very first known case of human monkeypox. I detailed this ridiculous situation more in-depth at viroLIEgy.com and I will provide the relevant articles in the recommended reading section.
The convenient emergence of monkeypox was a great way to cover up the fact that the same symptoms associated with smallpox still existed. It also offered the ability to cover-up the deadly vaccine injuries as well.
However, monkeypox was not the only new disease which popped up with the exact same smallpox symptoms. According to Dr. Viera Scheibner (PhD), a retired scientist and author, there were other similar diseases used as a scapegoat for the dangerous and ineffective vaccine:
Belief not science is behind flu jab promotion, new report says
“Harmful reactions and ineffectiveness of smallpox vaccination motivated the “eradication” campaign of the 1970s. Smallpox was pronounced eradicated on 8th May 1980, vaccination stopped and epidemics disappeared, bar small outbreaks of whitepox, buffalopox, monkeypox, camelpox and similar names, while the disease was indistinguishable from smallpox. According to Arita and Gromyko (1982. Bull WHO; 60 (4): 367-375), the main benefit of smallpox being pronounced officially eradicated was that vaccination could be discontinued in all countries. Simply, smallpox vaccination had become an embarrassment.”
Dr. Scheibner pointed out that buffalopox, whitepox, camelpox, and other diseases with similar names and symptoms began to appear in the place of smallpox. However, she didn't factor in that smallpox was also regularly confused with measles, chickenpox, scarlett fever, rubella, herpes, shingles, etc. since its conception in 1751 as a separate disease. Each of these conditions result in the same symptoms of disease with very minute “differences” said to distinguish them. At one point in time, they were all considered varying stages of the same disease process. None of these diseases can be clinically distinguished and diagnosed accurately based on symptoms alone due to these similarities, thus the need for nonspecific antibody results and/or fraudulent molecular tests today to rule in or out one or the other. Breaking the same symptoms into separate diseases is not only a great way to lower case counts to improve the perception of vaccine effectiveness, it also serves the purpose of creating more fear of the invisible boogeymen now spreading and mutating from animals to humans. This results in the demand and need for different pharmaceuticals, vaccinations, and treatments to “cure” each condition, which obviously makes for a great business model.
Polio Reclassified
Unlike smallpox, polio has not yet been “eradicated” by vaccines even though there have been two different vaccines available since the 1950's. However, as was observed previously, polio cases decreased dramatically before the introduction of these miracle “cures.”
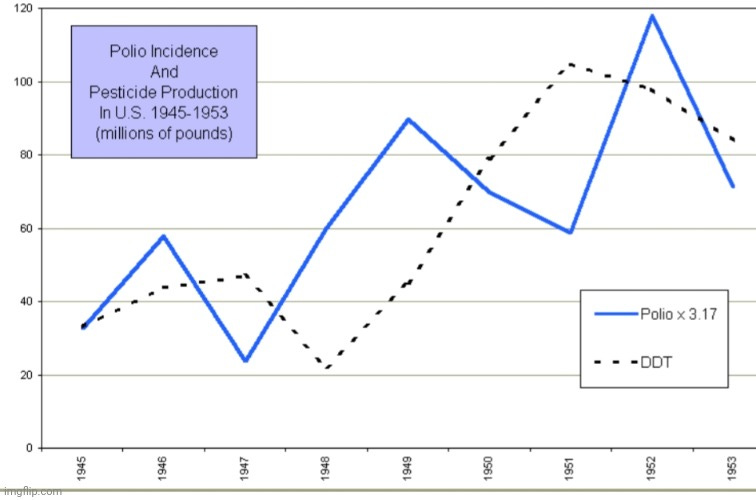
Thus, the reduction in polio cannot be attributed to the Salk vaccine campaign introduced in 1955 nor the Sabin oral vaccine in 1959. What could have contributed to the serendipitous drop in polio cases beyond the improved sanitation and clean food and water? One possibility was the gradual discontinuation of dangerous pesticides and insecticides such as DDT which concerned parents neglectfully sprayed on their children to combat polio. In 1949, Morton S. Biskind, M.D. wrote a paper looking at the effects of DDT on animals and humans. He spoke of the mysterious and elusive “Virus X” which was appearing more frequently each year with the increased use of DDT. This disease sounded quite a bit like polio and according to Dr. Biskind, it was easily confused with the disease due to the findings of damage to the central nervous system:
DDT Poisoning and the Elusive "Virus X."' A New Cause for Gastro-Enteritis
“DURING A PERIOD of more than two years, numerous cases of a curious symptom complex, apparently never before reported, have been observed throughout the United States. For want of a satisfactory explanation for this ailment, it has been widely attributed to infection with a thus far illusory "virus X.”
The syndrome consists of a group of or all the following: Acute gastroenteritis occurs, with nausea, vomiting, abdominal pain, and diarrhea usually associated with extreme tenesmus. Coryza, cough and persistent sore throat are common, often followed by a persistent or recurrent feeling of constriction or a "lump" in the throat; occasionally the sensation of constriction extends substernally and to the back and may be associated with severe pain in either arm. In some cases, the hyoid bone becomes acutely painful to pressure for a few days. Pain in the joints, generalized muscle weakness and exhausting fatigue are usual; the latter are often so severe in the acute stage as to be described bv some patients as "paralysis." Sometimes the initial attack is ushered in by vertigo and syncope. Intractable headache and giddiness are not uncommon. Occasionally herpes zoster appears.Paresthesia of various kinds occur in most of the cases; areas of skin become exquisitely hypersensitive and after a few days this hyperesthesia disappears only to recur elsewhere, or irregular numbness, tingling sensations, pruritus or formication may occur. Erratic fibrillary twitching of voluntary muscles is common. Usually there is diminution of vibratory sense in the extremities.”
“The high incidence, the usual absence of a febrile reaction, the persistence and erratic recurrence of the symptoms, the lack of observable inflammatory lesions, and the resistance even to palliative therapy, suggested an intoxication rather than an infection. Investigation for possible etiologic agents soon led to consideration of DDT (2, 2 bis (para-chlorophenyl) 1, 1, 1-trichloroethane; less precisely designated di-chlorodiphenyltrichloroethane). The epidemic first appeared at about the time DDT came into widespread use by the civilian population. The signs and symptoms described in tile pharmacologic and" toxicologic literature as characteristic of DDT poisoning, are identical with those appearing in patients with the affection described (1, to 13).”
“As already indicated, a prominent feature in virtually all the patients was extreme apprehensiveness. This is probably explicable on the basis of functional and possibly even morphologic changes in the central nervous system produced by DDT, since in DDT poisoning in animals such disturbances are frequent.*
* Needless to say, findings related to the nervous system, and muscular spasm and weakness in severe acute affections of this type. have led to confusion with such entities as meningitis and poliomyelitis.
Researcher Jim West did a lot of work uncovering this connection between polio symptoms and pesticides. In a 2004 paper, he outlined more from Dr. Biskind where the doctor linked DDT to the same degeneration of the anterior horn cells attributed to polio:
Pesticides and Polio: A Critique of Scientific Literature
‘Biskind also describes physiological evidence of DDT poisoning that resembles polio physiology:
“Particularly relevant to recent aspects of this problem are neglected studies by Lillie and his collaborators of the National Institutes of Health, published in 1944 and 1947 respectively, which showed that DDT may produce degeneration of the anterior horn cells of the spinal cord in animals. These changes do not occur regularly in exposed animals any more than they do in human beings, but they do appear often enough to be significant.”
He continues, bearing his exasperation in trying to make the obvious plain.
“When the population is exposed to a chemical agent known to produce in animals lesions in the spinal cord resembling those in human polio, and thereafter the latter disease increases sharply in incidence and maintains its epidemic character year after year, is it unreasonable to suspect an etiologic relationship?”
Jim West's article touches on other toxins such as BHC and lead-arsenic as potential contributing factors involved in the rising symptoms of polio along with DDT. Based on his painstaking research and meticulously plotted graphs, it is clear that there was a rise and fall in polio cases as the use of these toxins were introduced and then gradually reduced and phased out. According to the Environmental Protection Agency, DDT regulations began in the 1950's ending with the cancellation of the use of the toxic pesticide in the US in 1972. If one wanted to create the appearance that the vaccines were a miracle cure, reducing exposure to toxins that cause the exact same symptoms of the disease targeted is a good place to start:
“The U.S. Department of Agriculture, the federal agency with responsibility for regulating pesticides before the formation of the U.S. Environmental Protection Agency in 1970, began regulatory actions in the late 1950s and 1960s to prohibit many of DDT's uses because of mounting evidence of the pesticide's declining benefits and environmental and toxicological effects. The publication in 1962 of Rachel Carson's Silent Spring stimulated widespread public concern over the dangers of improper pesticide use and the need for better pesticide controls.
In 1972, EPA issued a cancellation order for DDT based on its adverse environmental effects, such as those to wildlife, as well as its potential human health risks.
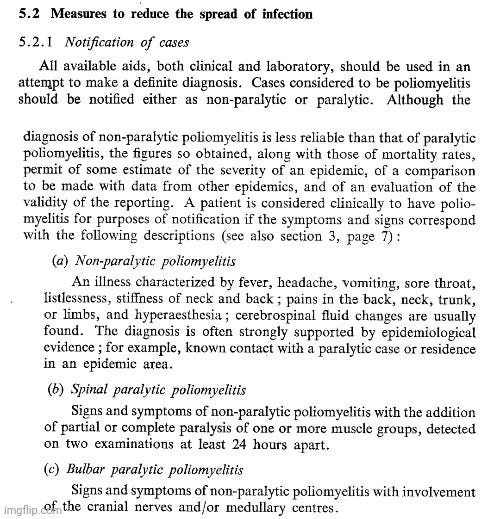
However, there was an even more obvious trick that was utilized in order to create the perception that polio cases declined with the introduction of the vaccines. Prior to the 1955 vaccination campaign, the WHO laid out the guidelines for how to make a diagnosis of either non-paralytic or paralytic polio in 1953. It was crucial for the WHO to make this distinction between cases that resulted in paralysis and those that did not for the ultimate success of the vaccination campaign, as will be shown later. In order to diagnose non-paralytic polio, the usual flu-like symptoms were all that were necessary to make a diagnosis even though this was considered less reliable than when confirming cases of paralytic polio. In those instances, all that was required to diagnose a patient with paralytic polio was the presence of the same flu-like symptoms as well as partial or complete paralysis upon two examinations carried out 24 hours apart. In neither non-paralytic nor paralytic polio were laboratory results necessary for a confirmation of a case:
https://apps.who.int/iris/handle/10665/40241
In a 1956 bulletin by the WHO, it was admitted that at least two-thirds of the cases diagnosed as non-paralytic polio were in fact not polio and were instead caused by other “viruses” and bacteria. Thus, it was important that, for a case to be considered polio, paralysis must occur as this was seen as a defining feature and indicative of polio. This paralysis requirement stood even though it was admitted that there are other causes of paralysis. The separation of polio into those with and without paralysis was necessary as the vaccine was said not to be effective at preventing non-paralytic polio and was only effective at reducing paralytic polio. If these two conditions could not be separated, it would obscure the “beneficial effects” of the vaccination campaign:
Poliomyelitis in 1954
“A variable proportion, which may be up to two-thirds or more, of cases diagnosed as non-paralytic poliomyelitis, presenting the clinical picture of aseptic meningitis, is due to other viruses (mumps, Coxsackie B, ECHO-6, Herpes simplex, LCM, various members of group A and group B encephalitis viruses, and others as yet undefined) as well as to bacteria (leptospirosis).”
“Clinical disease resembling paralytic poliomyelitis may be due to other viruses (see the reports from Iceland, Egypt, and Massachusetts). RSSE may also cause confusion.9 But there is little doubt that apart from relatively infrequent episodes the great majority of paralytic cases are due to poliovirus. For this reason and because paralysis is the result of poliovirus infection, which is of major public health importance, it has been repeatedly stressed by the World Health Organization that the incidence of paralytic and non-paralytic cases should be reported separately. There are many countries where this is still not yet done. This will become increasingly important as poliomyelitis vaccination comes into wider use, since the evidence available so far suggests that the main result of vaccination is to decrease the number of paralytic cases, the number of non-paralytic cases being relatively unaffected. Unless the two groups can be separated the beneficial effect of vaccination may be obscured.”
It can be seen that there was a concentrated effort to separate the symptoms of non-paralytic polio into many conditions caused by other “viruses” and bacteria, including:
Mumps
Coxsackie B
ECHO-6
Herpes Simplex
LCM
Other non-polio “enteroviruses”
Leptospirosis
Other unknown “viruses”
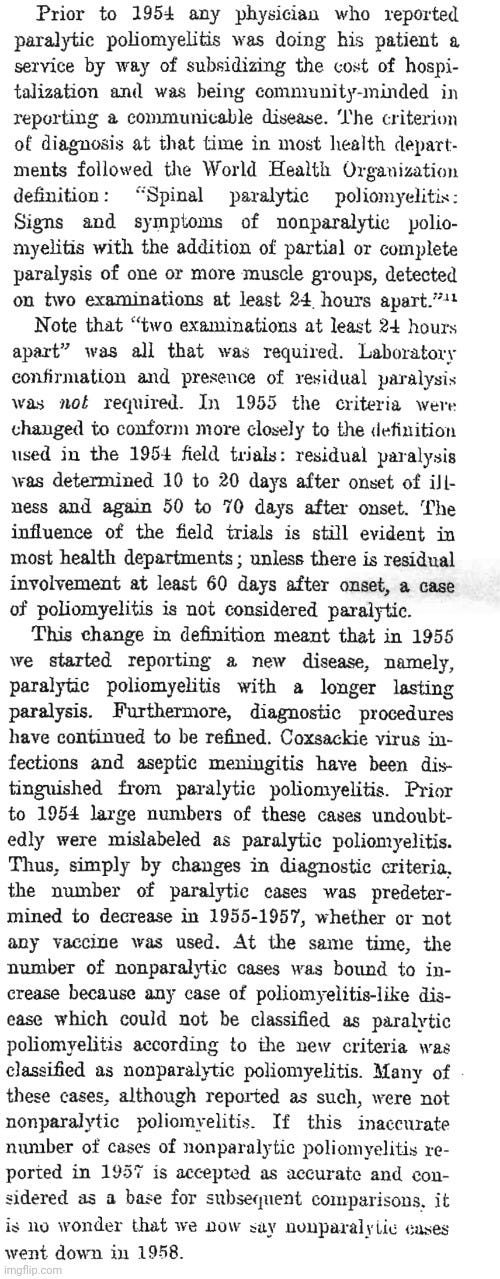
We can also see that they were beginning to make a distinction between cases of paralysis caused by the polio “virus” as well as those said to be caused by other “viruses.” This separation would be utilized to decrease cases later. For now, polio was successfully divided into those cases with paralysis and those without. Once this distinction was accepted, another nifty trick was instigated in order to create the appearance that the vaccine was even more effective. According to a 1955 report by Thomas Francis, Jr. regarding the polio vaccine trials, the criteria for how a paralytic polio case was diagnosed changed from those listed by the WHO in 1953. Instead of only requiring the confirmation of paralysis on two examinations 24 hours apart to diagnose paralytic polio, a confirmation was now based on two examinations spread further apart: one at 10-20 days and another at 50-70 days. A confirmation also now included reports on “virus isolation,” tests of antibody titer, and laboratory diagnosis which were not required in 1953. The ability to diagnose a case of paralytic polio was now a lot more difficult for a physician. Still, even with all of these new diagnostic measures in place, Francis Jr. admitted that there were difficulties in decisions due to contradictory results:
Evaluation of the 1954 Poliomyelitis Vaccine Field Trial
“The second phase in the evaluation was concerned with discovery and identification of all cases of poliomyelitis or suspected poliomyelitis in all children of the first, second, and third grades in the study areas. The various steps in the investigation of a case are: (1) physician's diagnosis—report to local health department; (2) telegraphic report to vaccine evaluation center; (3) action of local health department, including (a) clinicoepidemiological investigation and report to vaccine evaluation center, form FT-6, (b) collection and shipment of laboratory specimens (or by laboratory) and notice to vaccine evaluation center, form FT-9, and (c) notification of physical therapist; (4) first muscle evaluation by physical therapist (10 to 20 days) and physician's interpretation of patient's status, form FT-7; (5) collection of convalescent serum for laboratory, form FT-9; (6) second muscle evaluation by physical therapist (50 to 70 days) and physician's interpretation of patient's entire illness, form FT-8; (7) report of virus isolation, tests of antibody titer, laboratory diagnosis, form FT-10; (8) establishment and application of criteria for diagnosis of individual patient; and (9) integration of all data into final vaccine evaluation center diagnosis.
The criteria for diagnosis of poliomyelitis, for designation of a case as paralytic and its severity, and for the interpretation of laboratory results were carefully drawn. In this we had the continued help of an advisory committee comprised of expert clinicians, virologists, biostatisticians, epidemiologists, and administrators. The information concerning each case was carefully reviewed and the diagnostic classification made without knowledge of its vaccination status so that objectivity was readily maintained. Inevitably, difficulties in decision were encountered when results from different pieces of data were not in agreement, but the effort was made to follow a consistent plan of interpretation.”
The reason that this change in how paralytic polio was diagnosed is important was summarized by Dr. Bernard G. Greenberg. He testified to Congress in 1962 that the reduction in polio cases was not brought about by vaccination but was instead due to the adoption of this redefinition of the paralytic polio diagnosis. By spreading out paralysis to 60 days and beyond, a new long-lasting paralytic polio disease was created:
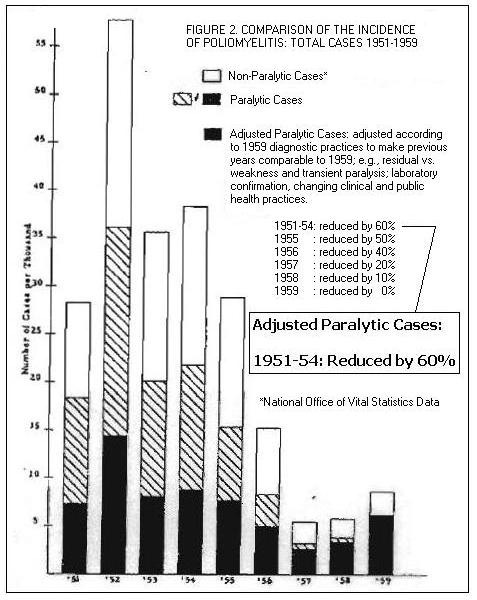
As can be seen from Dr. Greenberg, the change in diagnostic criteria for polio was all that was necessary in order to see a drop in paralytic polio. No vaccine was ever necessary. And to help sell this point, a graph was provided applying the new diagnostic criteria to polio cases from 1951 to 1959 which showed how the drop would have occurred had this criterion been used before the vaccine became available:
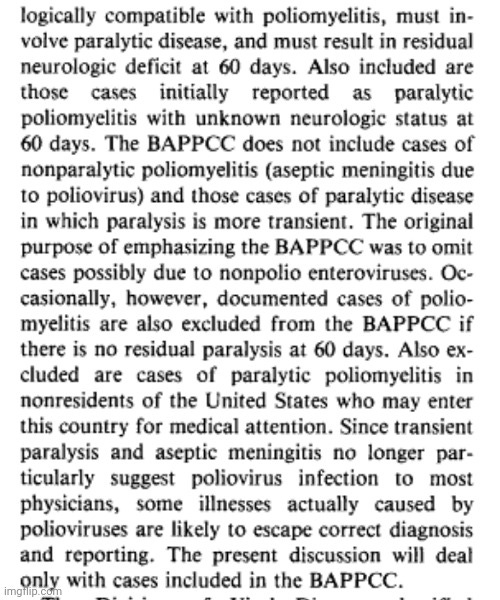
In order to confirm that the adoption of the vaccine trial diagnostic criteria was in fact used when reporting vaccine effectiveness and paralytic polio case numbers, we can turn to the book Poliomyelitis Surveillance. It indeed confirms this to be the case as the CDC officially counted paralytic polio cases according to the “best available paralytic poliomyelitis case count,” or BAPPCC. This count required that paralysis occurs up to 60 days. If there was no residual paralysis at 60 days, the cases were excluded from the count:
In 1969, the CDC officially adopted this 60-day requirement as the case definition for paralytic polio:
“ACIP. Poliomyelitis prevention. MMWR 1982;31:22-6, 31-4. *Since 1969, the CDC definition of a case of paralytic poliomyelitis has been a patient with paralysis clinically and epidemiologically compatible with poliomyelitis who, at 60 days after onset of symptoms, has a residual neurologic deficit, has died, or for whom no information is available on neurologic residua.”
It should be clear now that the change in diagnostic criteria for paralytic polio was the driving factor in reducing polio cases in an attempt to prop up the effectiveness of the toxic vaccines. However, this redefinition could not eliminate the symptoms of polio and wipe them from existence. As these symptoms would still persist, polio-related diseases such as aseptic meningitis and coxsackie were branched off into their own categories:
The polio vaccine: a critical assessment of its arcane history, efficacy, and long-term health-related consequences
“Doctors and scientists on the staff of the National Institutes of Health during the1950s were well aware that the Salk vaccine was causing polio. Some frankly stated that it was “worthless as a preventive and dangerous to take [26:142].” They refused to vaccinate their own children [26:142]. Health departments banned the inoculations [26:140]. The Idaho State Health Director angrily declared: “I hold the Salk vaccine and its manufacturers responsible” for a polio outbreak that killed several Idahoans and hospitalized dozens more [26:140]. Even Salk himself was quoted as saying: “When you inoculate children with a polio vaccine you don’t sleep well for two or three weeks [26:144;43].” But the National Foundation for Infantile Paralysis, and drug companies with large investments in the vaccine coerced the U.S. Public Health Service into falsely proclaiming the vaccine was safe and effective [26:142-5].”
“Polio is virtually nonexistent in the United States today. However, according to Dr. Robert Mendelsohn, medical investigator and pediatrician, there is no credible scientific evidence that the vaccine caused polio to disappear [50]. From 1923 to 1953, before the Salk killed-virus vaccine was introduced, the polio death rate in the United States and England had already declined on its own by 47 percent and 55 percent, respectively (Figure 4) [51]. Statistics show a similar decline in other European countries as well [51]. And when the vaccine did become available, many European countries questioned its effectiveness and refused to systematically inoculate their citizens. Yet, polio epidemics also ended in these countries [50].
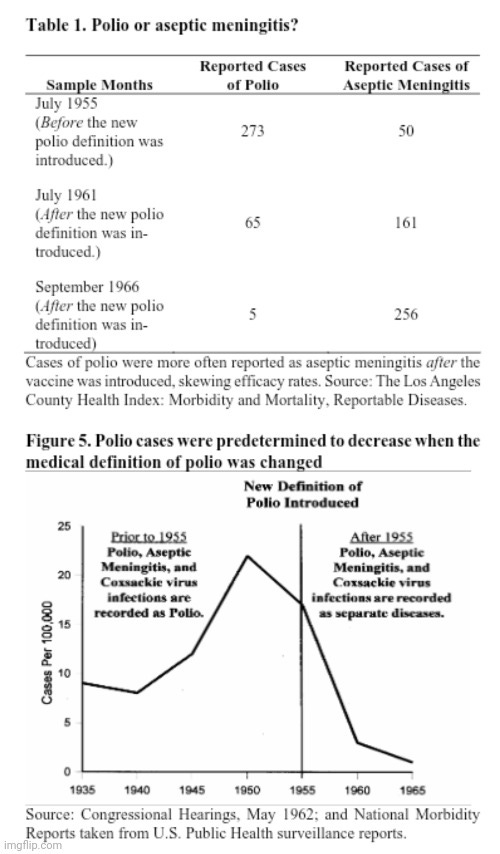
The standards for defining polio were changed when the polio vaccine was introduced. The new definition of a polio epidemic required more cases to be reported. Paralytic polio was redefined as well, making it more difficult to confirm, and therefore tally, cases. Prior to the introduction of the vaccine the patient only had to exhibit paralytic symptoms for 24 hours. Laboratory confirmation and tests to determine residual paralysis were not required. The new definition required the patient to exhibit paralytic symptoms for at least 60 days, and residual paralysis had to be confirmed twice during the course of the disease. Also, after the vaccine was introduced cases of aseptic meningitis (an infectious disease often difficult to distinguish from polio) and coxsackie virus infections were more often reported as separate diseases from polio. But such cases were counted as polio before the vaccine was introduced. The vaccine’s reported effectiveness was therefore skewed (Table 1 and Figure 5) [52,53].”
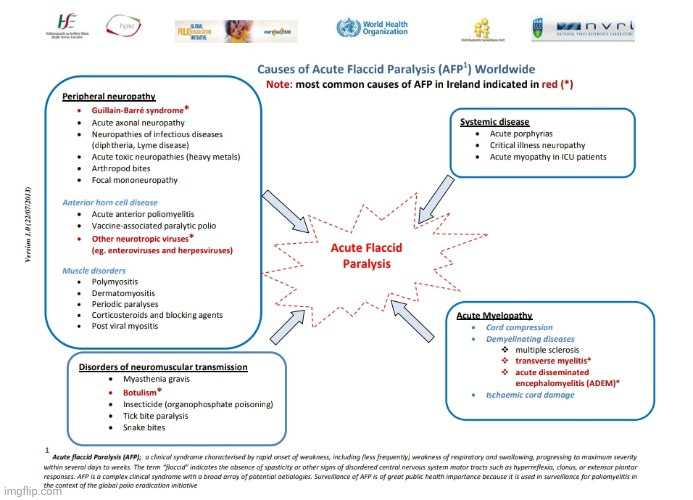
Old polio-associated diseases such as aseptic meningitis and coxsackie “virus” were broken away from polio in order to siphon off the cases previously diagnosed as such. Other conditions also appeared and became more frequently pegged as the culprit of paralysis instead of polio such as Guillain-Barre syndrome, acute traumatic neuritis, enteroviral myelitis, myopathy, etc. Even rabies, tetanus, and the West Nile “virus” are associated with the same symptoms of disease. For many decades, acute flaccid paralysis was the name for cases of polio as this was the defining condition of the disease. However, even though the two labels are interchangeable, an effort has been made over the decades to try and distinguish the two from each other. Now, it is stated that as polio (a.k.a. acute flaccid paralysis) goes away, AFP will stick around due to non-polio “enteroviruses” and other causes such as novel recombinant “viruses.” In other words, the same symptoms are being shifted away from the polio “virus” and onto other suspects:
Polio will go, acute flaccid paralysis will stay
“But as the Global Polio Eradication Initiative and the scientific community plan to celebrate polio eradication sooner or later, there is need for recognition that the risk of acute flaccid paralysis due to other enteroviruses is still high.
Acute flaccid paralysis is a weakness in one or more limbs or the respiratory or bulbar muscles, resulting from damaged lower motor neurons. The most common viral causes are polio and non-polio enteroviruses. As polio gradually disappears globally, there is major concern about the probable emergence of other neurotropic enteroviruses to occupy the niche and cause infections mimicking acute paralytic poliomyelitis. Enterovirus 71 for example has been regarded as the second most important neurotropic enterovirus, causing frequent outbreaks of paralytic disease. A crude mortality rate of 16% in children younger than 14 years was observed during an enterovirus 71 outbreak between 1998 and 2005 in Taiwan. Also, and equally important, is recombination between vaccine-derived poliovirus and other enteroviruses, which might result in the emergence of novel recombinant viruses causing similar paralytic diseases. Over the past decades, several non-polio enteroviruses have been discovered and some implicated in acute flaccid paralysis of unprecedented severity.”
More recently, a condition known as acute flaccid myelitis has made its presence felt. This is a relatively new disease that was “discovered” in 2010. It is an offshoot of acute flaccid paralysis, which for all intents and purposes was paralytic polio until 2010. Now, AFM has successfully taken over the title as it is defined as poliomyelitis not caused by the polio “virus,” thus it is yet another condition that is used to explain away cases of poliomyelitis still occurring today. The only difference separating the two diseases are the results from fraudulent laboratory tests which must be confirmed by an “expert” panel. In other words, AFM can be referred to as either non-polio polio or, my personal favorite, incognito polio:
How is AFM different from polio?
“Poliomyelitis is the term used to describe the syndrome of acute flaccid limb weakness and lesions in the grey matter of the spinal cord. Poliomyelitis caused by poliovirus, or polio, rarely occurs in the United States. In 2014, the term AFM was adopted to describe poliomyelitis without a known cause and not caused by poliovirus. AFM has some similarities with polio, such as the lesions in the grey matter of the spinal cord and flaccid limb weakness that can result in paralysis. Polio can be prevented by a vaccine.
Stool specimens that we receive from AFM patients are tested for poliovirus. If poliovirus is detected, it is considered a case of polio, not a case of AFM. We continue to test all specimens from AFM patients to look for viruses, including poliovirus and non-polio enteroviruses.”
“All suspected cases of paralytic poliomyelitis are reviewed by a panel of expert consultants before final classification occurs. Confirmed cases are then further classified based on epidemiologic and laboratory criteria.”
Hopefully the magic tricks utilized to create the appearance of the effectiveness of the vaccines has become clearer now and will no longer be effective to persuade anyone on the fence. When a “virus” needs to be either eradicated or minimized, all it takes is hiding the symptoms of disease under various names and disguises with either a new “viral” and/or bacterial cause. This decrease can also be helped along by reducing or eliminating environmental toxins associated with the same symptoms of disease and by changing the diagnostic criteria in order to make diagnosis less likely as seen in the case with polio.
We have seen this same situation with “Covid-19.” When the flu and other respiratory “viruses” needed to disappear for ‘Covid” to emerge, the symptoms were lumped into “Covid” along with many other unrelated ailments. Remember “Covid toes” and MIS-C, a.k.a. frostbite and Kawasaki disease? Cases of all “non-Covid” diseases dropped dramatically, even cancers and heart attacks. However, once the vaccine needed to be shown to be effective, “Covid” cases decreased while the “flu” and “RSV” re-emerged along with other respiratory diseases and ailments. They can keep this magic trick going as long as we continue to get hoodwinked by their theatrics. However, if you can see past the illusions, they will have to come up with new tricks in order to fool you. Let's continue to unveil their deceptions until they have nothing left to pull out of their hat.
Merchants of Doubt is highly recommended -- an entertaining documentary about intentional sleight of hand shenanigans by Big Tobacco, etc. https://www.sonyclassics.com/merchantsofdoubt/
Top 5 books I read in past 3 years (highly recommended):
Another possible cause of "polio" could be found, historically, in wallpaper. The following from an article in Nature, 12 June 2003, titled "William Morris made poisonous wallpaper" The quote, "Andy Meharg of the University of Aberdeen in Scotland has found arsenic in the green pigment in an early sample of Morris's patterned wallpaper, produced some time between 1864 and 1875. Such pigments were suspected even in the mid-nineteenth century of releasing toxic fumes if they become damp." Polio is poisoning. Thanks Mike, this one deserves a reread!











Merchants of Doubt is highly recommended -- an entertaining documentary about intentional sleight of hand shenanigans by Big Tobacco, etc. https://www.sonyclassics.com/merchantsofdoubt/
Top 5 books I read in past 3 years (highly recommended):
https://WhatReallyMakesYouIll.com/
https://drtomcowan.com/products/Breaking-the-Spell-the-Scientific-Evidence-for-Ending-the-Covid-Delusion?variant=41299699204249
https://ourfreesociety.com/viruses/Virus-Mania-torsten-engelbrecht.pdf (https://VirusManiaFilms.com/)
https://openlibrary.org/books/OL8435090M/Good-Bye_Germ_Theory
https://archive.org/details/the-real-anthony-fauci-bill-ga-robert-f.-kennedy
Another possible cause of "polio" could be found, historically, in wallpaper. The following from an article in Nature, 12 June 2003, titled "William Morris made poisonous wallpaper" The quote, "Andy Meharg of the University of Aberdeen in Scotland has found arsenic in the green pigment in an early sample of Morris's patterned wallpaper, produced some time between 1864 and 1875. Such pigments were suspected even in the mid-nineteenth century of releasing toxic fumes if they become damp." Polio is poisoning. Thanks Mike, this one deserves a reread!