



Breakthrough:
a sudden advance especially in knowledge or technique
an act or instance of moving through or beyond an obstacle
Almost three years ago, we were sold a scarytale about the fearsome new “virus” that was quickly approaching from a far off distant land. This new threat was coming to claim our elderly, our children, and our sickly for its rapidly rising death toll. Temporary “protective” measures were put into place as barriers to defend us from the outside invader. However, we were told that, even though they were meant to flatten an imaginary curve in only a few short weeks, these restrictions would not be enough to contain the threat and would only slow it down. In order to save ourselves and those we love, it was imperative that we submit to a rushed experimental injection that would infuse each individual with a protective shield known as immunity. We were told that as more people willingly submitted themselves to these hastily thrown together mystery injections and we reached a certain threshold, the protective shield would expand and create a super barrier known as herd immunity. We were ensured that this selfless act would afford our community protection, immunity, and stop the transmission of this deadly foe in its very tracks.
The high priests overseeing the creation of this mystical elixir made many promises about their products and stated that once one gets vaccinated, they will be afforded some level of protection that will prevent infection which would stop the “virus” from spreading amongst the population. Those vaccinated would also not succumb to severe disease nor hospitalization if they were to somehow aquire the “virus.” However, were these promises based on actual scientific data or were they merely sleazy sales tactics to get as many jabs in as many arms as quickly as possible before the truth finally came out? The beauty of hindsight is that we can look back and see the many marvelous claims which were made about the exceptional benefits afforded to those who accepted these products, and we can also see that these promises were nothing but dishonest lies that never came to fruition and were all but abandoned as the “breakthrough” cases and the evidence piled up.
The Promise:
Let's start this journey by looking back at the early days of the “pandemic” in order to see what amazing powers were said to be granted by these magical elixirs. In July 2020, Anthony Fauci met with Congress to assure the public that the vaccines would protect everyone by stopping infections and transmissions thus preventing future outbreaks:
“Fauci urged everyone to get vaccinated for COVID-19 to protect themselves as well as others from infection — to stop transmission and prevent future outbreaks. While the process of developing a vaccine has been among the fastest on record, Fauci assured people that the "prudent but rapid" process remained safe while undergoing clinical trials.”
In an August 2020 interview with NIH Director Francis Collins, Fauci stated that it was assumed that the vaccines would offer some sort of finite protection. How long this protection would last, they did not know. However, Fauci did claim that once one was infected “naturally,” they did not become re-infected. In fact, he said such an occurrence was rare, thus oddly implying that natural “infection” afforded protection which logicallly would make the use of an experimental vaccine pointless. One can only surmise then that the promised vaccines, which are supposedly superior and more effective than “natural” infection at affording protection and combating re-infection, would make such a “rare” occurence non-existent:
Excerpts from NIH Director Dr. Francis Collins' conversation with Dr. Anthony Fauci, director of NIH's National Institute of Allergy and Infectious Disease.
“Collins: Okay, so suppose this all looks really good and you have a vaccine that’s safe and effective, and we start immunizing people. How long will that protection last when you’ve got a vaccine? Are you going need to take it again?
Fauci: We do not know the answer to that. I mean, you can assume that you’re going to get protection at least to take us through this cycle. When you look at natural infection it’s anywhere between six months to a year.… We’re going to assume that there’s a degree of protection, but we have to assume that it's going to be finite. It’s not going to be like a measles vaccine. So there’s going to be follow-up in those cases to see if we need a boost. We may need a boost to continue the protection. But right now we do not know how long it lasts.
Collins: And do we know whether people who got natural infection with this virus SARS-CoV-2 can get re-infected? Are there cases where people really got better and then got sick again?
Fauci: There are no documented cases where people got better and actually got sick again in the sense of virus replicating (multiplying). They were able to do PCR (a test to detect the virus’s genetic material) of what was likely viral fragments that showed up on PCR. The idea of relapses, I wouldn’t be surprised if there’s a rare case of an individual who went into remission and relapse.…But, … I could say with confidence that it is very unlikely….”
https://newsinhealth.nih.gov/2020/08/dr-anthony-fauci-covid-19-vaccines
In an letter to the world, Pfizer CEO Albert Bourla seemingly agreed with Fauci that the vaccines would offer protection and that it would prevent disease in the majority of those vaccinated. He laid out the three criteria that they needed to meet in order to get Emergency Use Authorization for their vaccine, which not only included preventing disease but also proven safety:
“There are three key areas where, as with all vaccines, we must demonstrate success in order to seek approval for public use. First, the vaccine must be proven effective, meaning it can help prevent COVID-19 disease in at least a majority of vaccinated patients. Second and equally important, the vaccine must be proven safe, with robust safety data generated from thousands of patients. And finally, we must demonstrate that the vaccine can be consistently manufactured at the highest quality standards.”
https://www.pfizer.com/news/articles/an_open_letter_from_pfizer_chairman_and_ceo_albert_bourla
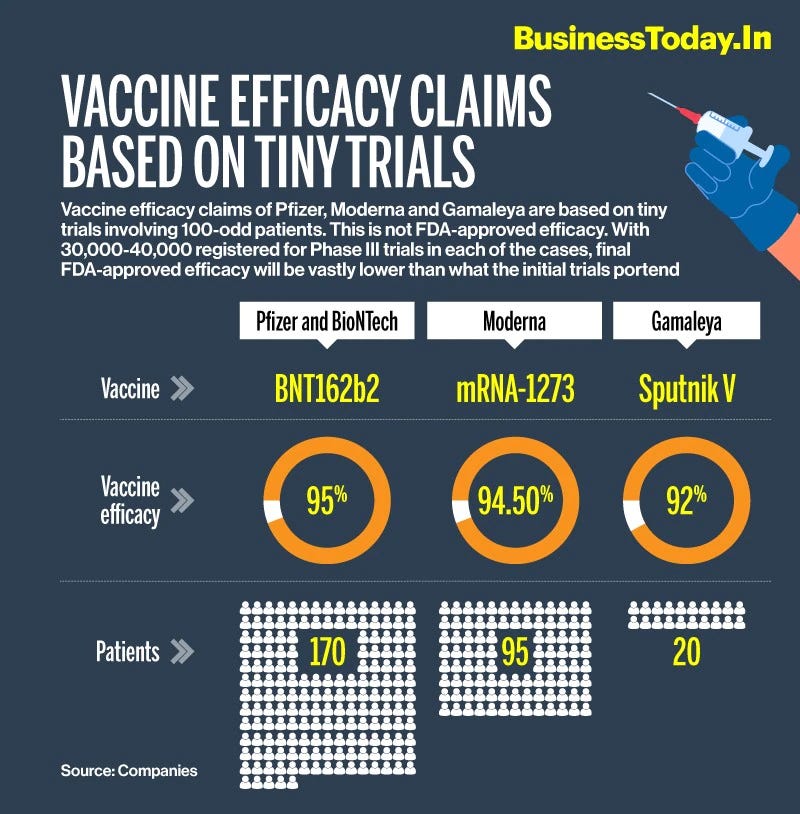
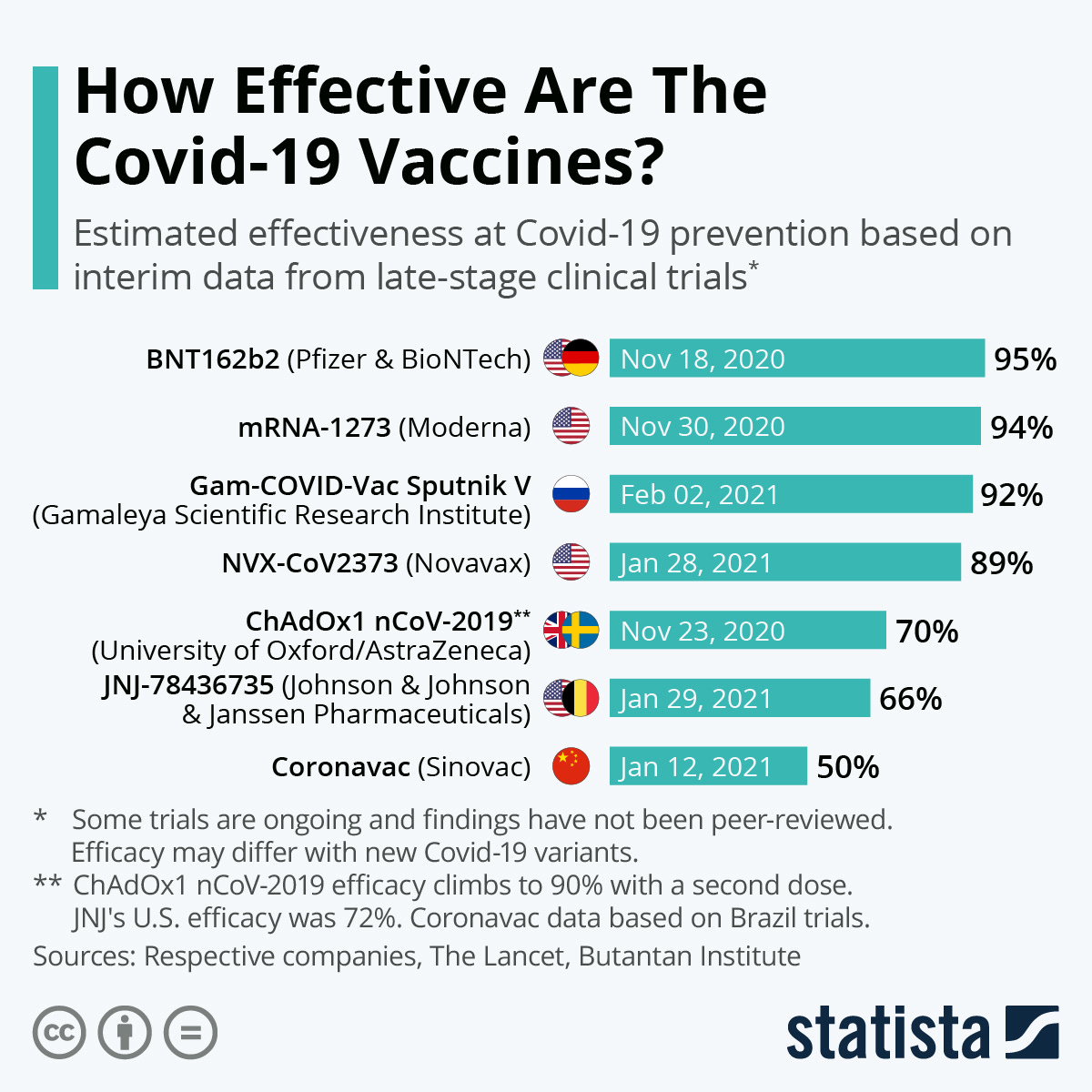
Pfizer later claimed to meet its goals by stating that the vaccine was 95% efficacious at preventing “Covid-19” infections and that it caused no serious safety concerns:
“A final analysis of the Phase 3 trial of Pfizer's coronavirus vaccine shows it was 95% effective in preventing infections, even in older adults, and caused no serious safety concerns, the company said Wednesday.”
In a December 2020 interview, Moderna CEO Stephane Bancel stated that they were optimistic that their vaccine would also protect people and reduce transmission:
“So we're cautiously optimistic that our vaccine should be able not only to protect people who receive it from disease, but also protect the community by reducing spreading.”
https://www.advisory.com/blog/2020/12/moderna-ceo-covid-vaccine-bancel
In fact, Moderna stated that their vaccine was 94% effective at preventing “Covid-19” which, according to Bancel, was a “game-changer.” He also claimed that not only could his vaccine prevent “Covid-19,” it could prevent severe disease:
“Moderna said preliminary phase three trial data shows its coronavirus vaccine is more than 94% effective in preventing Covid-19 — a result CEO Stephane Bancel called a “game changer.”
“Since early January, we have chased this virus with the intent to protect as many people around the world as possible. All along, we have known that each day matters,” he said in a statement. “This positive interim analysis from our Phase 3 study has given us the first clinical validation that our vaccine can prevent COVID-19 disease, including severe disease.”
In November 2020, Anthony Fauci stated that getting vaccinated not only protected the person getting vaccinated, but that it also protected ones family and community by preventing the spread of the “virus.” According to Fauci, the vaccinated are a “dead-end” for the “virus” as it has no where to go to infect anyone else:
“When you get vaccinated, you not only protect your own health and that of the family but also you contribute to the community health by preventing the spread of the virus throughout the community,” Fauci said. “In other words, you become a dead end to the virus. And when there are a lot of dead ends around, the virus is not going to go anywhere. And that’s when you get a point that you have a markedly diminished rate of infection in the community.”
In December 2020, Anthony Fauci predicted that the US would begin to see the effects of the invisible protective shield forming around the vaccinated by April or May of 2021. This shield, known as herd immunity, was long considered the main objective of getting as many vaccinated as quickly as possible:
Fauci Predicts U.S. Could See Signs Of Herd Immunity By Late March Or Early April
“Dr. Anthony Fauci, the nation's senior official for infectious diseases, predicts the United States could begin to achieve early stages of herd immunity against the deadly coronavirus by late spring or summer. And if that happens, Fauci anticipates, "we could really turn this thing around" toward the end of 2021.
In a wide-ranging interview Tuesday on Morning Edition, NPR's Rachel Martin asked Fauci how many Americans need to receive the vaccine to have an impact on the number of COVID-19 infections.
"I would say 50% would have to get vaccinated before you start to see an impact," Fauci said. "But I would say 75 to 85% would have to get vaccinated if you want to have that blanket of herd immunity."
“Fauci said if all goes according to plan, by the end of March or beginning of April more vaccines will be available to the general public.
"Once we get there, if in the subsequent months, April, May, June, July, we get as many people vaccinated as possible, we could really turn this thing around before we get towards the end of the year," Fauci said.
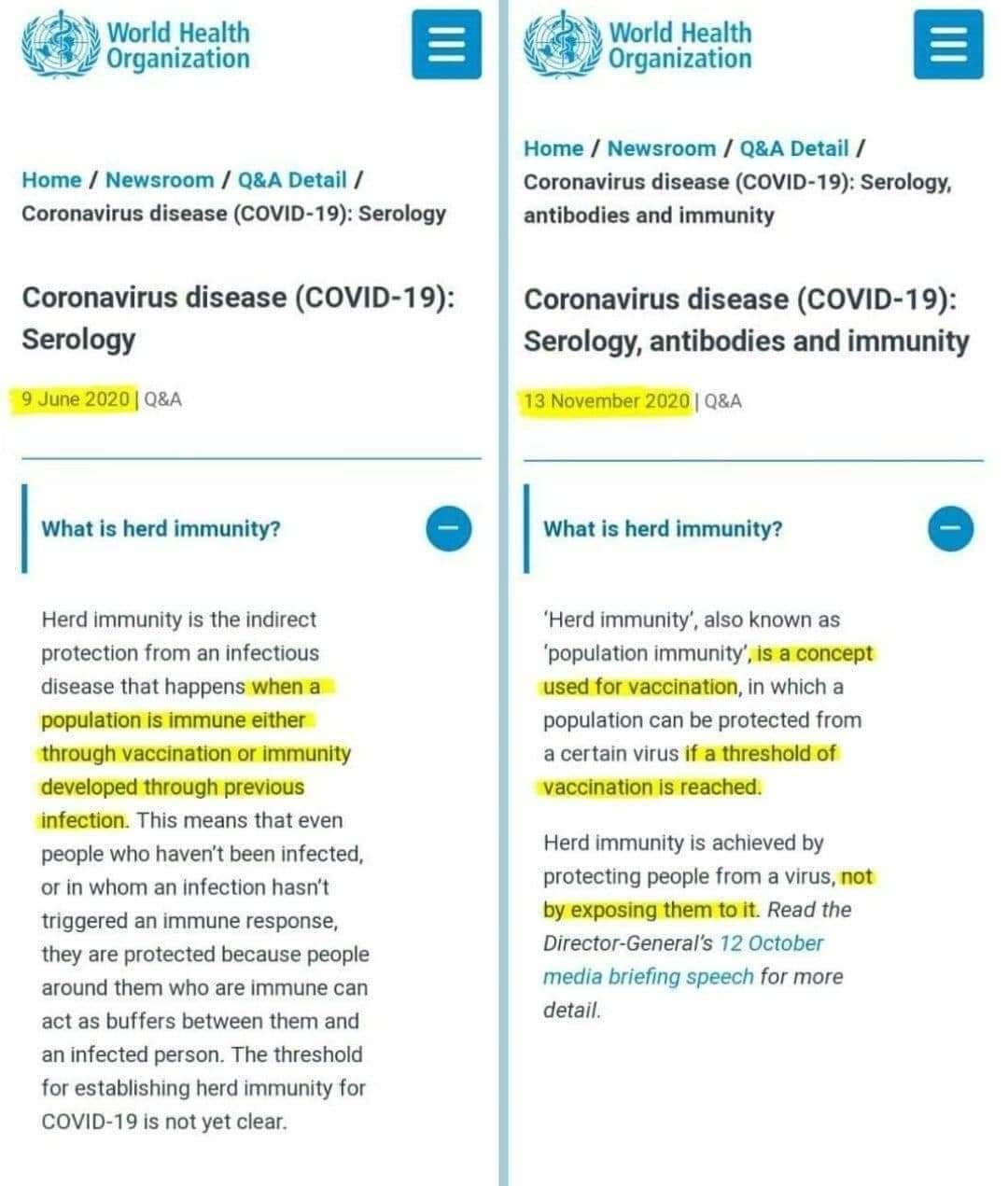
At some point between June and November 2020, the WHO made the subtle change to the definition of herd immunity by moving it away from any sort of immunity aquired through natural “infection” and/or vaccination to instead only being able to be achieved through the process of vaccination:
It is clear from the statements of the people involved with the creation of these experimental concoctions that those who lined up for their injection would:
Be granted some sort of protection which would prevent infection
Avoid severe disease and hospitalization
Prevent the transmission of the “virus” to loved ones and the community
Once aquired, this defensive aura would wrap around the population, creating the mythical herd immunity that would lead to a dead end for the “virus” which would ultimately trample the foe down to a miniscule or possibly non-existent threat. However, somewhere along the line, the grandiose promises made by the high priests began to fade as chinks in the armor started to appear.
The Renege:
As soon as late December 2020, Anthony Fauci admitted to moving the goal posts for what it would ultimately take in order to achieve immunity for the herd, bumping his estimates from a low of 70% on up to 90%:
NYT: Fauci acknowledges moving goalposts on herd immunity from COVID-19
"When polls said only about half of all Americans would take a vaccine, I was saying herd immunity would take 70 to 75 percent ... Then, when newer surveys said 60 percent or more would take it, I thought, "I can nudge this up a bit," so I went to 80, 85. We need to have some humility here .... We really don’t know what the real number is. I think the real range is somewhere between 70 to 90 percent. But, I'm not going to say 90 percent."
https://www.axios.com/2020/12/25/fauci-goalposts-herd-immunity
Less than a year later, the CDC began to abandon the concept of herd immunity altogether, stating that it may not be possible as the vaccines had not proved reliable in regards to stopping transmission. Instead of the shield protecting the people from getting the “virus,” success would now be gauged on how many became infected and whether they died afterwards. In other words, there would be no immunity for the herd:
CDC shifts pandemic goals away from reaching herd immunity
“Since the earliest days of the pandemic, there has been one collective goal for bringing it to an end: achieving herd immunity. That’s when so many people are immune to a virus that it runs out of potential hosts to infect, causing an outbreak to sputter out.
Many Americans embraced the novel farmyard phrase, and with it, the projection that once 70% to 80% or 85% of the population was vaccinated against COVID-19, the virus would go away and the pandemic would be over.
Now the herd is restless. And experts at the Centers for Disease Control and Prevention have set aside herd immunity as a national goal.
The prospects for meeting a clear herd-immunity target are “very complicated,” said Dr. Jefferson Jones, a medical officer on the CDC’s COVID-19 Epidemiology Task Force.
“Thinking that we’ll be able to achieve some kind of threshold where there’ll be no more transmission of infections may not be possible,” Jones acknowledged last week to members of a panel that advises the CDC on vaccines.
Vaccines have been quite effective at preventing cases of COVID-19 that lead to severe illness and death, but none has proved reliable at blocking transmission of the virus, Jones noted. Recent evidence has also made clear that the immunity provided by vaccines can wane in a matter of months.
The result is that even if vaccination were universal, the coronavirus would probably continue to spread.
“We would discourage” thinking in terms of “a strict goal,” he said.”
“The CDC’s new approach will reflect this uncertainty. Instead of specifying a vaccination target that promises an end to the pandemic, public health officials hope to redefine success in terms of new infections and deaths — and they’ll surmise that herd immunity has been achieved when both remain low for a sustained period.”
By March 2022, Anthony Fauci completely reversed course on achieving “classical” herd immunity in an article published in The Journal of Infectious Diseases by stating that the concept was “unattainable” for “Covid-19.” He oddly claimed that vaccines struggled to control other “more controllable” respiratory “viruses” such as smallpox, long considered the only “virus” to be eradicated by vaccination. He admitted that “Covid-19” vaccination did not offer prolonged protection and then provided a laundry list of reasons why herd immunity was unattainable. It seemed that the “dead-end” the “virus” was to face which would stop transmission was more of an annoyance than an actual barrier:
The Concept of Classical Herd Immunity May Not Apply to COVID-19
“There are significant obstacles to achieving complete herd immunity with COVID-19. Classical herd immunity, leading to disease eradication or elimination, almost certainly is an unattainable goal. As noted, mass vaccination and aggressive public health approaches have struggled to control other (seemingly more controllable) respiratory infectious diseases, such as smallpox, measles, and rubella, all caused by viruses with limited phenotypic evolution. Controlling SARS-CoV-2 and its cycles of new variants presents a much more formidable challenge [23]. Like influenza, SARS-CoV-2 mutates continually into new variants that can escape immunity derived from infections and vaccines. It also can be transmitted asymptomatically and without pathognomonic signs, impeding public health control. SARS-CoV-2 appears not to substantially engage the systemic immune system, as do viruses such as smallpox, measles, and rubella that consistently have a pronounced viremic phase. Moreover, neither infection nor vaccination appears to induce prolonged protection against SARS-CoV-2 in many or most people. Finally, the public health community has encountered substantial resistance to efforts to control the spread of SARS-CoV-2 by vaccination, mask wearing, and other interventions.”
“Thus, COVID-19 is likely to be with us, even if at a very low level of endemic community spread and with lower severity, for the foreseeable future. Like influenza, any level of herd protection against SARS-CoV-2 potentially can be overcome by ever-changing levels of immunity among countless subpopulations, by human movement, crowding, changes in social or prevention behaviors, by demographics, by vaccination levels, by variations in durability of infection- or vaccine-induced immunity, and by evolution of viral variants, among many other variables.”
“Living with COVID-19 is best considered not as reaching a numerical threshold of immunity, but as optimizing population protection without prohibitive restrictions on our daily lives. Effective tools for prevention and control of COVID-19 (vaccines, prevention measures) are available; if utilized, the road back to normality is achievable even without achieving classical herd immunity.”
https://academic.oup.com/jid/article/226/2/195/6561438?login=false
As the herd immunity lie crumbled apart, we started to see that the once miraculous claims of 95-100% efficacy quickly began to fall in the proceeding months after the vaccines launched. Efficacy is defined as the ability to produce an intended result. According to the WHO, a vaccines efficacy is “measured in a controlled clinical trial and is based on how many people who got vaccinated developed the ‘outcome of interest’ (usually disease) compared with how many people who got the placebo (dummy vaccine) developed the same outcome.” Thus, this efficacy number reflects ideal controlled conditions. According to the CDC, the goal was to understand how this idealized efficacy metric fared in the “real-world,” which is considered the vaccines effectiveness:
“After the U.S. Food and Drug Administration (FDA) approves a vaccine or authorizes a vaccine for emergency use, experts continue to assess vaccine effectiveness—or how a vaccine works in real-world conditions. The goal is to understand how a vaccine protects people outside of strict clinical trial settings.”
In other words, everyone who willingly subjected themselves to the experimental vaccine because they heard the vaccine had 95% efficacy did so based on idealized metrics in strictly controlled conditions. They were then used as guinea pigs to determine if this number actually held up. Once the vaccine was released into the wild without these idealized conditions, the efficacy numbers plummeted as it was shown that the vaccine did not, in fact, provide the intended result. A study published in The Lancet in October 2021 found that the claimed efficacy rate tumbled down from a high of 89% to 47% after six months:
Pfizer/BioNTech COVID-19 vaccine effectiveness drops after 6 months, study shows
“The effectiveness of the Pfizer Inc (PFE.N)/BioNTech SE vaccine in preventing infection by the coronavirus dropped to 47% from 88% six months after the second dose, according to data published on Monday that U.S. health agencies considered when deciding on the need for booster shots.”
Another study published around the same time showed the efficacy levels dropping to 20%:
Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar
“BNT162b2-induced protection against infection builds rapidly after the first dose, peaks in the first month after the second dose, and then gradually wanes in subsequent months. The waning appears to accelerate after the fourth month, to reach a low level of approximately 20% in subsequent months.”
https://www.nejm.org/doi/full/10.1056/NEJMoa2114114?query=featured_home
As the efficacy rate fell, so too did the effectiveness rate of the vaccine. Effectiveness refers to the degree of success in being able to produce the desired result. According to the WHO, the vaccines effectiveness is a “measure of how well vaccines work in the real world.” As clinical trials “cannot be a perfect representation of the whole population,” the efficacy seen in these trials only “applies to specific outcomes in a clinical trial.” The WHO admitted that the effectiveness in the real world can differ from the efficacy measured in a clinical trial because they “can’t predict exactly how effective vaccination will be for a much bigger and more variable population getting vaccinated in more real life conditions.” In other words, they were selling the frightened population on the amazing 95-100% efficacy rates in order to convince them to take the experimental plunge. They had no idea if this “game-changing” number reflected reality. In fact, this efficacy has not been achieved in the real world setting and this waning efficacy has been reflected in dwindling effectiveness rates. The CDC's own July 2022 study showed effectiveness rates as low as 24%:
“To evaluate effectiveness of 2, 3, and 4 doses of mRNA COVID-19 vaccines (Pfizer-BioNTech or Moderna) among adults with healthy immune systems, experts examined VISION Network data on more than 214,000 emergency department/urgent care visits and more than 58,000 hospitalizations with a COVID-19–like illness diagnosis in 10 U.S. states from mid-December 2021 through mid-June 2022. Study findings show:
When BA.1 was the predominant variant, vaccine effectiveness (VE) was 61% for two doses against COVID-19-associated hospitalizations; VE increased to between 85%–92% after receipt of a third/booster dose.
When BA.2/BA.2.12.1 became predominant, vaccine effectiveness with two doses was 24% against COVID-19-associated hospitalizations and increased to 52%–69% after a third/booster dose.
Patterns were similar for emergency department and urgent care encounters, with lower VE during BA.2/BA.2.12.1 predominance and higher VE with 3 or 4 doses compared to VE with 2 doses.
Among adults ages 50 years and older during BA.2/BA.2.12.1, vaccine effectiveness against COVID-19–associated hospitalization was 55% more than 4 months after a booster/third dose and increased to 80% more than a week after the fourth dose
https://www.cdc.gov/media/releases/2022/s0715-COVID-VE.html
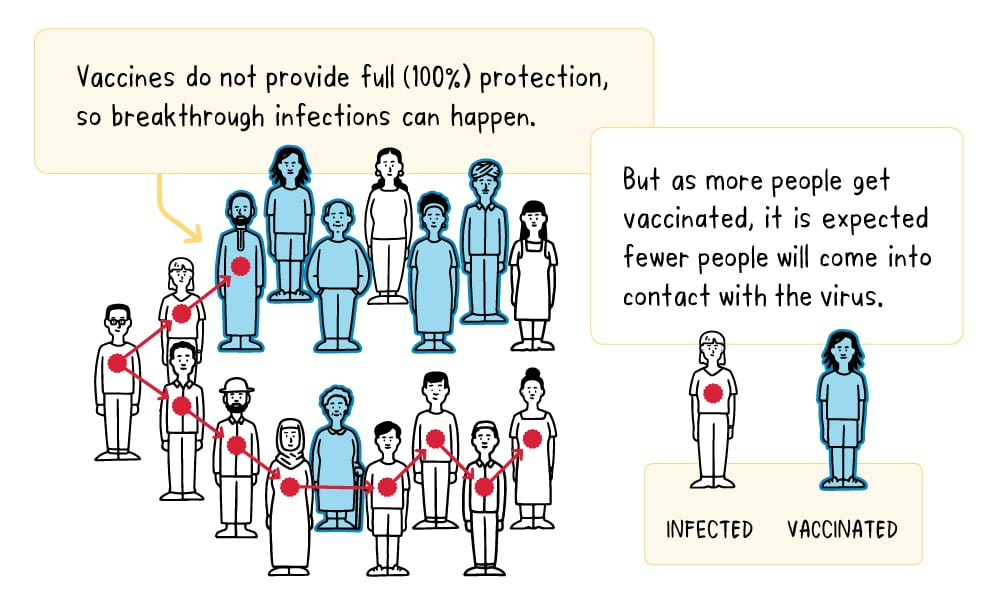
As the vaccines were unable to achieve the promised efficacy rates and have shown to have sub-par effectiveness rates, it should come as no surprise that the “infections” continued to be detected even amongst the vaccinated. The shield of protection was not all that it was meant to be due to the emergence of breakthrough cases in the vaccinated. In May 2021, the CDC admitted that breakthrough infections were expected until enough people became vaccinated in order to achieve the desired immunity level…invoking the same herd immunity concept that they would abandon a few months later. They claimed that even though these cases occurred in the vaccinated, it was in only a small fraction:
“Even though FDA-authorized vaccines are highly effective, breakthrough cases are expected, especially before population immunity reaches sufficient levels to further decrease transmission. However, vaccine breakthrough infections occur in only a small fraction of all vaccinated persons and account for a small percentage of all COVID-19 cases (5–8). The number of COVID-19 cases, hospitalizations, and deaths that will be prevented among vaccinated persons will far exceed the number of vaccine breakthrough cases.”
https://www.cdc.gov/mmwr/volumes/70/wr/mm7021e3.htm
However, it really was not only a “small fraction” of the vaccinated being “diagnosed” with “Covid” as, according to the CDC's own partner in crime The Johns Hopkins Institute, a breakthrough rate of 1 in 100 fully vaccinated individuals testing positive for “Covid” was seen recently in some populations:
Can you get COVID after being vaccinated?
“Yes. Breakthrough COVID-19 cases happen in people who are fully vaccinated, and they seem to happen more frequently now that the delta variant is circulating widely and immunity may be waning among those who got the vaccine many months ago. All three available coronavirus vaccines are very good at protecting you against severe forms of COVID-19, but they are not 100% effective in preventing infection. Breakthrough COVID can be caused by the delta variant, which is more contagious than some other coronavirus variants.
How common are breakthrough cases of COVID?
A study in Washington state gathered data from over 4 million fully vaccinated people. The data showed a rate of about 1 in 5,000 experienced a breakthrough infection between January 17 and August 21, 2021. More recently, some populations have shown breakthrough infection rates of approximately 1 in 100 fully vaccinated people.”
Times Magazine wrote an article stating that it was time to rethink breakthrough infections as these were not “rare” occurences, especially in light of the go-to excuse of the “more contagious variants:”
We Need to Start Thinking Differently About Breakthrough Infections
Rare no longer
“A lot remains to be learned about Omicron, but the U.S. Centers for Disease Control and Prevention (CDC) has warned that it is likely to cause breakthrough infections. Early studies suggest COVID-19 vaccines will continue to dramatically limit severe disease and death, but may not be as good at preventing symptomatic disease caused by Omicron, compared to other strains. The variant also arrived at an inopportune time, when vaccine-related immunity was starting to wane for people who had gotten their shots early in the year and hadn’t yet been boosted.
https://www.google.com/amp/s/time.com/6130704/breakthrough-infections-omicron/%3famp=true
Even vaccine-maker AstraZeneca had to admit that these cases are common when there is a lot of illness or “virus” circulating, even though this is exactly what the vaccine was supposed to prevent. Why was it unsuccessful? You guessed it. “Variants:”
Are breakthrough infections common?
“Breakthrough infections become more frequent when there is a lot of illness or virus circulating in a community. When cases increase and virus transmission accelerates, it is more likely that new virus variants will emerge that may be more contagious. These can lead to more infections overall, contributing to an increased frequency of breakthroughs occurring.”
https://www.astrazeneca.com/what-science-can-do/topics/covid-19/breakthrough-infections.html
In June 2022, the CDC had to agree and admitted that the breakthrough “infections” will occur even if the vaccination levels are high, thus destroying any reason to get vaccinated in order to “protect the community.” The vaccinated can still get “Covid” and speard it to others. In fact, in communities with high “Covid” cases, it doesn't matter whether one is vaccinated or not as they must continue wearing an ineffective mask to cover up for the equally ineffective vaccine:
“COVID-19 vaccines help protect against severe illness, hospitalization and death. COVID-19 vaccines also help protect against infection. People who are vaccinated may still get COVID-19. When people who have been vaccinated get COVID-19, they are much less likely to experience severe symptoms than people who are unvaccinated.”
“People who get vaccine breakthrough infections can spread COVID-19 to other people. When a community reports more COVID-19 infections, that means more virus is circulating. When more virus is circulating, more breakthrough infections will occur even when vaccination rates are high. Even if you are vaccinated, if you live in a county with a high COVID-19 Community Level, you and others in your community, whether vaccinated or not, should take more steps to protect yourself and others, like wearing a mask in indoor public places.”

By July 2022, after having tested positive for “Covid” even though he was quadruple vaccinated and boosted, Anthony Fauci had to admit that the vaccines do not protect people overly well from infection. He tried to argue that the vaccines are able to protect against severe disease and hospitalizations yet, as pointed out in the linked article, recent data does not support his statement:
“In an effort to argue that the COVID-19 vaccines still have some virtue, President Biden’s chief medical adviser said out loud what had become clear to most of the world, that the shots don’t protect people from infection as was promised.
Dr. Anthony Fauci – who tested positive for COVID-19 last month after being quadruple vaccinated – acknowledged Tuesday to the Fox News Channel’s Neil Cavuto that the vaccines “don’t protect overly well” from infection.
“One of the things that’s clear from the data [is] that even though vaccines – because of the high degree of transmissibility of this virus – don’t protect overly well, as it were, against infection, they protect quite well against severe disease leading to hospitalization and death,” Fauci said.
However, an analysis of Pfizer and Moderna COVID vaccine trials found the mRNA shots are more likely to land a recipient in the hospital than to provide protection from a severe adverse event. The findings were similar to those of a recent pre-print analysis that found “no evidence of a reduction in overall mortality in the mRNA vaccine trials.” And a new study published in the New England Journal of Medicine found that two doses of the mRNA vaccines increased the risk of COVID-19 infection during the omicron wave.”
All of this information may leave one wondering how the promises made by those promoting their own products went so wrong. How did this rushed experimental elixir fail to live up to the various grandiose claims made of it? Perhaps it is because the studies meant to provide the information on the effectiveness of the vaccines were not designed to properly evaluate any of the claims made. This was pointed out in October 2020 by senior editor of The BMJ Peter Doshi. In his article, he noted that every measure of success promised by the makers of the toxic injections, from preventing infection and deaths to stopping transmission, were not studied during the clinical trials as they were never intended to evaluate these things:
Will covid-19 vaccines save lives? Current trials aren’t designed to tell us
“As phase III trials of covid-19 vaccines reach their target enrolments, officials have been trying to project calm. The US coronavirus czar Anthony Fauci and the Food and Drug Administration leadership have offered public assurances that established procedures will be followed.1234 Only a “safe and effective” vaccine will be approved, they say, and nine vaccine manufacturers issued a rare joint statement pledging not to prematurely seek regulatory review.5
But what will it mean exactly when a vaccine is declared “effective”? To the public this seems fairly obvious. “The primary goal of a covid-19 vaccine is to keep people from getting very sick and dying,” a National Public Radio broadcast said bluntly.6
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”7
Yet the current phase III trials are not actually set up to prove either (table 1). None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.”
“But Tal Zaks, chief medical officer at Moderna, told The BMJ that the company’s trial lacks adequate statistical power to assess those outcomes. “The trial is precluded from judging [hospital admissions], based on what is a reasonable size and duration to serve the public good here,” he said.
Hospital admissions and deaths from covid-19 are simply too uncommon in the population being studied for an effective vaccine to demonstrate statistically significant differences in a trial of 30 000 people. The same is true of its ability to save lives or prevent transmission: the trials are not designed to find out.
Zaks said, “Would I like to know that this prevents mortality? Sure, because I believe it does. I just don’t think it’s feasible within the timeframe [of the trial]—too many would die waiting for the results before we ever knew that.”
Stopping transmission
“What about Hotez’s second criterion, interrupting virus transmission, which some experts have argued17 should be the most important test in phase III studies?
“Our trial will not demonstrate prevention of transmission,” Zaks said, “because in order to do that you have to swab people twice a week for very long periods, and that becomes operationally untenable.”
“Zaks pointed to influenza vaccines, saying they protect against severe disease better than mild disease. To Moderna, it’s the same for covid-19: if its vaccine is shown to reduce symptomatic covid-19, it will be confident it also protects against serious outcomes.
But the truth is that the science remains far from clear cut, even for influenza vaccines that have been used for decades. Although randomised trials have shown an effect in reducing the risk of symptomatic influenza, such trials have never been conducted in elderly people living in the community to see whether they save lives.
Only two placebo controlled trials in this population have ever been conducted, and neither was designed to detect any difference in hospital admissions or deaths.23 Moreover, dramatic increases in use of influenza vaccines has not been associated with a decline in mortality (box 2).26”
https://www.bmj.com/content/371/bmj.m4037
In January 2021, Doshi wrote another article challenging the 95% efficacy rate supplied by Moderna. In it, he questioned why suspected “Covid” cases were not included in the efficacy data. Had they been included, that 95% efficacy rate would have collasped down to 19%, similar to what the CDC's own studies currently show:
Peter Doshi: Pfizer and Moderna’s “95% effective” vaccines—we need more details and the raw data
“All attention has focused on the dramatic efficacy results: Pfizer reported 170 PCR confirmed covid-19 cases, split 8 to 162 between vaccine and placebo groups. But these numbers were dwarfed by a category of disease called “suspected covid-19”—those with symptomatic covid-19 that were not PCR confirmed. According to FDA’s report on Pfizer’s vaccine, there were “3410 total cases of suspected, but unconfirmed covid-19 in the overall study population, 1594 occurred in the vaccine group vs. 1816 in the placebo group.”
With 20 times more suspected than confirmed cases, this category of disease cannot be ignored simply because there was no positive PCR test result. Indeed this makes it all the more urgent to understand. A rough estimate of vaccine efficacy against developing covid-19 symptoms, with or without a positive PCR test result, would be a relative risk reduction of 19% (see footnote)—far below the 50% effectiveness threshold for authorization set by regulators. Even after removing cases occurring within 7 days of vaccination (409 on Pfizer’s vaccine vs. 287 on placebo), which should include the majority of symptoms due to short-term vaccine reactogenicity, vaccine efficacy remains low: 29% (see footnote).”
How did the people pushing their rushed experimental injections not know that the guarantees that they pitched to the public were fraudulent? Their own studies were never designed to measure any of the benefits being claimed. In all available metrics, the promises made turned out to be flat out deceitful lies. Their magical elixir:
Did not prevent “infections”
Did not prevent transmission
Did not prevent severe hospitalizations and death
Did not create herd immunity
When factoring in the numerous cases of myocarditis, blood clots, strokes, bells palsy, anaphylaxis, and other severe reactions up to and including death as seen in those who unfortunately made the fateful decision to believe in those who promoted fear to sell the “cure,” it is clear that the vaccines failed in being a safe alternative as well. With the fall of the claimed benefits, the narrative shifted away from “the vaccines will prevent infections and stop transmission which will protect the community” to “everyone will get ‘Covid’ at some point but the vaccines will delay it and may make it mild.” The EUA for these vaccines was authorized on the basis that the known and unknown benefits outweighed the known and unknown risks. At this time, it is very clear that there are no known benefits yet there are plenty of known risks.

At the beginning of this article, I highlighted the definition of the word breakthrough to showcase its two meanings. One is in regards to overcoming a barrier. The fictional “SARS-COV-2” conveniently found a way to breatk through the invisible protective vaccine shield that was all but guaranteed to stop the “virus” in its tracks. At least that is the narrative we have been sold and that they will continue to sell with variants and boosters in order to keep the frightened trapped in a mental barrier that they must be able to free themselves of if they ever want to break away from this “viral” nightmare.
The way to do so is by focusing on the alternate definition for breakthrough which refers to an advancement in knowledge. Look back at the numerous claims made over the last few years and the consistent failures to live up to them as well as the various excuses used to cover up these dishonest statements. Then continue to reseatch the contradictory and fraudulent claims made as there is far more information out there than any one article could ever cover in its entirety. Use this article as a springboard for further research. It is time for those who made the mistake of believing in the magical promises to have their own breakthrough in knowledge. Upon researching, the realization will come that these experimental injections were never meant to do what they were promised to do. Once this advancement in knowledge is achieved, it will be possible to break through the pharmaceutical barrier built by deceitful lies and see this scam for what it has always been. It is time to have a “Covid” breakthrough amongst those still invested in the pharmaceutical propaganda in order to end this fear-based narrative once and for all.

Investigative journalist Eric Coppolino
wrote a fantastic piece detailing the beginnings of his questioning of the “Covid” scam and his subsequent investigation into the fraudulent PCR methods being used and abused to prop up this casedemic: wrote an excellent article critiquing the germ theory of disease, pointing out alternate explanations for why people may experience similar symptoms of dis-ease around the same time after getting together: released yet another amazing video, this time calling out the pied pipers promoting the gain of function fear-porn Boogie Nights-style:
https://odysee.com/@drsambailey:c/Virologie-Nights:5
Dr. Tom Cowan had a very engrossing conversation with German engineer Marvin Haberland which revolved around his upcoming court case in Germany as well as the foundations of virology. Dr. Cowan billed it as one of his most important podcasts he has ever done. I think it definitely lives up to the hype:
https://drtomcowan.com/blogs/podcasts/56-marvin-haberland
Researcher Kate Sugak interviewed ex-scientist
on his work with HIV and “antibodies.” It was a truly fascinating discussion that everyone should check out:https://odysee.com/@katie.su:7/mikedoniokatesugak:1

Share this post